

Timeliness of Salmonella Typhimurium notifications after the introduction of routine MLVA typing in NSW
Cherie Heilbronn A B D , Sally Munnoch A , Michelle T. Butler C , Tony D. Merritt C and David N. Durrheim CA OzFoodNet, Hunter New England Population Health
B Turning Point, Eastern Health, Victoria
C Hunter New England Population Health
D Corresponding author. Email: cherieh@turningpoint.org.au
NSW Public Health Bulletin 24(4) 159-163 https://doi.org/10.1071/NB13010
Published: 17 June 2014
Abstract
Salmonella Typhimurium is the most common bacterial cause of gastrointestinal disease in NSW. Regular review of surveillance procedures ensures system objectives are met and informs improvements in system utility and efficiency. This paper assesses the timeliness and data completeness of NSW Salmonella Typhimurium surveillance after the routine introduction of multilocus variable repeat analysis (MLVA), a rapid sub-typing technique. MLVA results were available significantly earlier than alternate sub-typing techniques over the 2 years of this review. Accordingly, from a timeliness perspective, MLVA offers a favourable Salmonella Typhimurium sub-typing option in NSW. Further opportunities to improve timeliness and data completeness are identified. This paper was produced as part of a review of Salmonella Typhimurium surveillance in NSW for the period 2008–2009 by members of OzFoodNet based at Hunter New England Population Health. OzFoodNet is a national network established by the then Commonwealth Department of Health and Ageing in 2000 to enhance foodborne disease surveillance in Australia.
Salmonella Typhimurium (STm) is the most common Salmonella serotype in New South Wales (NSW); in 2009 STm accounted for 54% of all NSW Salmonella notifications1 and 77% of Australian foodborne outbreaks with an identified causative agent.2 STm is a heterogeneous Salmonella serovar, requiring additional sub-typing to identify outbreak-specific strains. Research exploring sub-typing techniques proffers multilocus variable repeat analysis (MLVA) as a rapid alternative to phage typing,3,4 the sub-typing technique historically used in Australia. MLVA typing has been shown to successfully differentiate strains within phage types 135a and 170 that comprise more than half the STm isolates in NSW.5 In 2006 and 2007, routine STm MLVA sub-typing was implemented in Queensland and NSW, respectively.
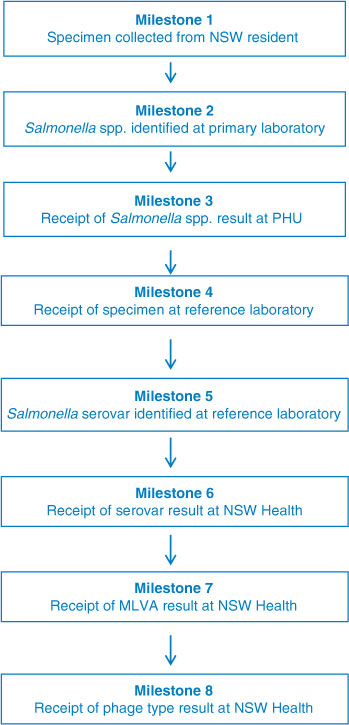
Regular review of public health surveillance determines the success of system objectives and informs refinement of system utility and efficiency.6,7 The NSW Salmonella surveillance system involves a complex network of local and interstate laboratories and notification processes. Local primary laboratories identify Salmonella species (spp.), while serovar confirmation and MLVA typing occur at the closest reference laboratory, and phage typing at one of the two national phage typing laboratories (Institute of Medical and Veterinary Science (IMVS), Adelaide and Medical Diagnostic Unit (MDU), Melbourne). The NSW Public Health Act 1991 (and its subsequent revision in 2010) mandates laboratories to notify all confirmed Salmonella cases. In 2008 and 2009 notifications were entered into the NSW Notifiable Diseases Database (NDD) by Public Health Units (PHUs) for data collation, timely outbreak detection and disease control, key objectives of the NSW surveillance system.8
This paper assesses the timeliness and completeness of NSW Salmonella Typhimurium surveillance data after the routine introduction of MLVA. Serovar and MLVA notifications received in 2008 and 2009 were reviewed to identify opportunities for minimising delays.
Methods
The Centers for Disease Control and Prevention’s Updated Guidelines for Evaluating Public Health Surveillance Systems6 were used as an evaluation framework for this investigation.
Data sources
STm notifications of NSW residents with a specimen collection date from 1 January 2008 to 31 December 2009 were identified and extracted in August 2010. As a new data management system (Notifiable Conditions Information Management System (NCIMS)) was instituted in May 2010, notifications were entered into the NDD during 2008 and 2009, but data were extracted from NCIMS in 2010. Additional milestone dates were obtained from the Institute for Clinical Pathology and Medical Research (ICPMR) electronic notifications and Queensland Health Forensic and Scientific Services (QHFSS), the NSW and Queensland reference laboratories, respectively. Other state reference laboratories were excluded as MLVA typing was not routinely conducted during the period of interest. NDD data comprised primary laboratory name and the date of Salmonella spp. receipt at the relevant PHU. ICPMR data included the following dates: specimen collection, Salmonella spp. identification, isolate receipt at ICPMR, and the electronic notification of serovar, MLVA and phage typing. The QHFSS dataset provided specimen collection date and the electronic notification dates of serovar and MLVA typing.
Data management and analysis
The relevant ICPMR and QHFSS dates were added to the NDD data extraction using SAS software (version 9.2, SAS Institute, Cary, NC, USA).
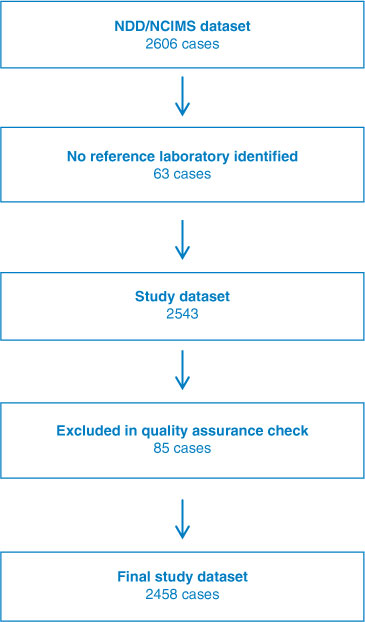
Eight milestones of public health importance were used in the analysis (Figure 1). Completeness and accuracy of milestones affected the number of cases available for timeliness evaluation; accordingly, a review of data completeness was conducted. Data cleaning verified the accuracy of extracted data and guided exclusion of duplicate cases and repeat specimens (specimens less than 14 days apart).8 Additional quality assurance checks involved scrutiny and possible exclusion of unexpected dates, established by negative time between sequential surveillance milestones. Time intervals greater than 365 days were reviewed to determine validity and excluded where appropriate. A total of 2458 cases (94.3% of all STm notifications) were included in the analysis (Figure 2).
|
|
SAS software and Microsoft Excel 2010 were used for quality assurance checks, calculation of time intervals between milestones, and significance testing, using Wilcoxon rank sum test methodology.
Results
Timeliness
The timeliness of all STm milestones, determined by the median interval in days, with the exception of receipt of phage typing, remained relatively consistent over time (Table 1). MLVA notification occurred 23 days earlier than phage typing in 2008 (p < 0.001) and 44 days earlier in 2009 (p < 0.001). The median time interval for MLVA notifications decreased significantly from 23 days in 2008 to 21 days in 2009 (2 days' decrease, p < 0.001).

|
Data completeness
Missing or invalid data were infrequent for most milestones, with a few notable exceptions (Table 2). The receipt of the initial Salmonella spp. report at PHU level was missing in 16.5% of cases and invalid in 1.3% of cases. Serovar identification date was missing in 5.4% of cases. Sub-typing was not recorded for a small number of STm cases, including 17 serovar, 33 MLVA and 88 phage type results.

|
Anomalies in sequential notification
Given the consecutive nature of STm typing, milestone notification for MLVA and phage typing are expected to occur after serovar availability. Time interval analysis indicated this was not always the case. Serovar and MLVA typing results were received simultaneously in 1% of cases in 2008 and 6% of cases in 2009.
Discussion
Regular evaluation of public health surveillance is important to confirm system utility and efficiency.6 To our knowledge, this is the first report of MLVA timeliness in the context of a population level STm surveillance system. MLVA results were available significantly earlier than phage typing results over the 2 years of this review. The availability of NSW MLVA results in 2008 (median 23 days) and 2009 (median 21 days) was also fast in comparison to phage typing in a similar timeliness study conducted in Ireland (median 25 days).9 Notably, median time to MLVA availability was shorter in 2009 than in 2008. This reduction during the third year of routine MLVA typing may be driven by increased efficiency as key players become accustomed to the MLVA process.
MLVA and phage typing notification was absent for a small number of cases. It is unclear whether typing was available but not reported or if typing was not conducted. One possible explanation is informed cessation of sub-typing when cases are epidemiologically linked to a known outbreak. However, as NDD data entry capabilities did not include case or outbreak linking during the study period, we cannot assess the impact of outbreak resolution on missing results.
Occasionally, laboratories did not notify sub-typing results at the earliest opportunity, as indicated by simultaneous or non-sequential notification of serovar, MLVA or phage typing results. While electronic notification via email is undoubtedly faster than postal mail, human errors in data collation and transmission between organisations are challenging to eliminate. Missing dates and notification sequence anomalies indicated notification lapses by primary laboratories. These data quality issues impact the day-to-day operational processes of outbreak identification, investigation and control. However, due to the complex nature of NDD data entry and extraction from NCIMS, further exploration of this issue was not possible.
Resourcing impacts the time interval from specimen collection to result availability. Phage typing is particularly affected as two reference laboratories (IMVS and MDU) service all Australian states. Phage type result timeliness may also be impacted by isolate ‘batching’, where isolate dispatch to the reference laboratory is delayed until a sufficient number of isolates are collated. Batching may have become more commonplace in NSW after the introduction of routine MLVA and an accompanying reduction in urgency for phage typing results. A previous study identified Salmonella spp. identification as the ‘bottle neck’ in the surveillance system,7 yet we found that the majority of Salmonella spp. identification occurred within 3 days. Also, the time interval from specimen collection to Salmonella spp. PHU notification was similar to a previous international timeliness study.9 Nonetheless, the additional median 4- (2008) or 3- (2009) day time interval from Salmonella spp. identification to PHU receipt provides an opportunity to reduce notification delays.
In 2010, the NDD was replaced with NCIMS, an updated data capture system with enhanced foodborne disease surveillance capacities. NCIMS capabilities include date stamping (identifying the date and time of data entry), outbreak case linking, and recording MLVA and phage typing results. NCIMS performance enhancements are expected to improve outbreak identification, establish historical sub-typing data banks, and advance future surveillance system evaluations through superior data quality. Indeed, capacity for real-time electronic importation of notifications directly into NCIMS (electronic laboratory reporting (ELR)) has been partially realised. In 2013, ELR was implemented by four laboratories conducting a substantial proportion of Salmonella spp. identification. The elimination of transmission delay and human error inherent in multiple data entry points may have already reduced time from Salmonella spp. identification to PHU receipt. However, an efficient data extraction method, to facilitate future timeliness and data quality evaluations, has not yet been developed.
Further opportunities to improve timeliness and data completeness include:
-
Dissemination of ELR across all laboratories, thereby reducing duplication of data entry and expediting data delivery.
-
Development of NCIMS capability for efficient data extraction and reporting relevant to future data completeness and timeliness evaluations. This would enable evaluation of NCIMS capacity to enhance the NSW STm surveillance system.
Limitations
Interpretation of our findings requires consideration of data limitations, including the use of secondary data collated for operational purposes. NDD data entry and NCIMS data extraction capabilities, surveillance system reliance on manual data entry at multiple laboratories and PHUs, and manual result dispatch from laboratories to health services, impacted data quality. To minimise this bias, staff scrutinised each record to assess data for exclusion as necessary.
Conclusion
Given the importance of rapid typing in outbreak responses and the endemic presence of STm in NSW, timely receipt of STm sub-typing is of public health importance. From a timeliness perspective, MLVA offers a favourable STm sub-typing option in NSW. Further, this project identified additional opportunities to enhance the STm surveillance system and improve enteric outbreak detection and control.
Acknowledgments
This work was funded by OzFoodNet and Hunter New England Population Health. OzFoodNet is a national network established in 2000 and funded by the then Commonwealth Department of Health and Ageing to enhance foodborne disease surveillance in Australia. We wish to acknowledge the contribution of Tracey Findlay for her role in data collation and cleaning. We would also like to thank our public health reference laboratory colleagues at ICPMR and QHFSS for their enthusiasm for MLVA typing and the provision of additional milestone data, as well as our colleagues at MDU and IMVS for phage typing.
References
[1] Kardamandis K, Heilbronn C, Munnoch S, McWeeny C, Stephens N. NSW 2009 OzFoodNet Annual Report. Available at: http://www.health.nsw.gov.au/Infectious/diseases/Documents/ofn_annual_report_2009.pdf (Cited 14 April 2014).[2] OzFoodNet Working Group Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: Annual report of the OzFoodNet Network, 2009. Commun Dis Intell 2010; 34 396–426.
[3] Lindstedt BA, Vardund T, Aas L, Kapperud G. Multiple-locus variable-number tandem-repeats analysis of Salmonella enterica subsp. enterica serovar Typhimurium using PCR multiplexing and multicolor capillary electrophoresis. J Microbiol Methods 2004; 59 163–72.
| Multiple-locus variable-number tandem-repeats analysis of Salmonella enterica subsp. enterica serovar Typhimurium using PCR multiplexing and multicolor capillary electrophoresis.Crossref | GoogleScholarGoogle Scholar | 1:CAS:528:DC%2BD2cXnslGitrc%3D&md5=10f4ab6446152e891904bac6248ba23dCAS | 15369852PubMed |
[4] Wang Q, Chiew R, Howard P, Gilbert G. Salmonella typing in New South Wales: current methods and application of improved epidemiological tools. N S W Public Health Bull 2008; 19 24–8.
| Salmonella typing in New South Wales: current methods and application of improved epidemiological tools.Crossref | GoogleScholarGoogle Scholar | 1:CAS:528:DC%2BD1cXhsVGhtrjI&md5=dca84fb02f29307053adefc1924b6945CAS | 18361865PubMed |
[5] Sintchenko V, Wang Q, Howard P, Ha CW, Kardamanidis K, Musto J, et al. Improving resolution of public health surveillance for human Salmonella enterica serovar Typhimurium infection: 3 years of prospective multiple-locus variable-number tandem-repeat analysis (MLVA). BMC Infect Dis 2012; 12 78
| Improving resolution of public health surveillance for human Salmonella enterica serovar Typhimurium infection: 3 years of prospective multiple-locus variable-number tandem-repeat analysis (MLVA).Crossref | GoogleScholarGoogle Scholar | 22462487PubMed |
[6] CDC; the Guidelines Working Group Updated Guidelines for Evaluating Public Health Surveillance Systems. MMWR 2001; 50 1–35.
| 18634202PubMed |
[7] Takahashi T, Koehler J, Swenson P, Duchin J. Evaluation of a public health Salmonella surveillance system in King County, Washington. Am J Infect Control 2004; 32 7–11.
| Evaluation of a public health Salmonella surveillance system in King County, Washington.Crossref | GoogleScholarGoogle Scholar | 14755228PubMed |
[8] Communicable Diseases Surveillance and Control Unit. NSW Notifiable Diseases Database Manual. 6th ed. Sydney: NSW Department of Health; 2002.
[9] Nicolay N, Garvey P, Delappe N, Cormican M, McKeown P. Completeness and timeliness of Salmonella notifications in Ireland in 2008: a cross sectional study. BMC Public Health 2010; 10 568
| Completeness and timeliness of Salmonella notifications in Ireland in 2008: a cross sectional study.Crossref | GoogleScholarGoogle Scholar | 20860803PubMed |