

Typhoid and paratyphoid fever in Western Sydney Local Health District, NSW, January–June 2011
Sarah J. Blackstock A , Vicky K. Sheppeard B , Jen M. Paterson B and Anna P. Ralph A C DA Blacktown Hospital, Blacktown
B Centre for Population Health, Western Sydney and Nepean Blue Mountains Local Health Districts
C Sydney Emerging Infections and Biosecurity Institute, The University of Sydney
D Corresponding author. Email: anna.ralph@sydney.edu.au
NSW Public Health Bulletin 23(8) 148-152 https://doi.org/10.1071/NB11041
Published: 21 September 2012
Abstract
We undertook a study of enteric fever, caused by Salmonella enterica enterica subtypes Typhi and Paratyphi A, presenting in residents of the Western Sydney Local Health District for the period January–June 2011. Twelve cases of S. Typhi and eight of S. Paratyphi A were notified. Patients were predominantly young adults (median age 26 years, 70% female) who had been visiting friends and relatives in India, Samoa, Bangladesh or Sri Lanka. No cases were associated with travel for less than 3 weeks; 17 (85%) required hospitalisation. None received pre-travel vaccination; reasons cited for this included pregnancy, expense, being too busy, or considering the disease too mild to warrant vaccination. Three S. Typhi isolates acquired at large social gatherings in Samoa had the same serotype and susceptibility profiles; these results were communicated to Samoan public health personnel. There are opportunities to strengthen enteric fever prevention, including pre-travel health advice and S. Typhi vaccination for people visiting endemic areas for 3 or more weeks, especially those in the vulnerable ‘visiting friends and relative’ category.
Enteric fever is caused by Salmonella enterica subspecies enterica serovars Typhi (S. Typhi) and Paratyphi (S. Paratyphi), with infection transmitted by the faecal-oral route.1,2 While uncommon in Australia due to public health measures, worldwide the disease accounts for significant morbidity and mortality in children and adults.3 A 2004 study estimated that 21 650 974 illnesses and 216 510 deaths occur each year caused by typhoid globally; paratyphoid accounts for an estimated 5 412 744 illnesses.2 Asia has the highest estimated typhoid incidence rates at 274 per 100 000 population, south-central Asia being the most heavily-burdened area within this region. The Pacific Islands are categorised as having moderate incidence.2,3
In Australia, enteric fevers are notifiable (i.e. hospitals and laboratories are required to report cases) and require extensive follow-up to prevent spread.4 Appropriate clinical management comprises administration of an antibiotic to which the isolate is susceptible (usually azithromycin or ceftriaxone) and the use of contact precautions.5 On notification to the public health unit, the source of the infection is established and risk examined, including whether the patient has an occupation that may allow transmission (e.g. food handling; carer for children, elderly people or those with impaired immunity). In such cases, the patient is required to abstain from work until follow-up stool specimens are culture negative. Household contacts are given hygiene advice and recommendations to provide stool specimens for screening. Contacts working in transmission-prone occupations are required to demonstrate two uninfected stool samples before resuming work.4
The Western Sydney Local Health District (LHD) of New South Wales (NSW) has a high proportion of migrants from typhoid-endemic areas. Residents born overseas comprise 31–59% of the populations in the five local government areas within the boundaries of the Western Sydney Local Health District, and 25–75% of the population of the LHD speak a language other than English at home.6 Foreign-born Australians visiting friends and relatives in their country of origin are well known to bear a disproportionate burden of the imported cases of enteric fever and other travel-related infections. Despite previous awareness-raising efforts, this group remains at risk.7
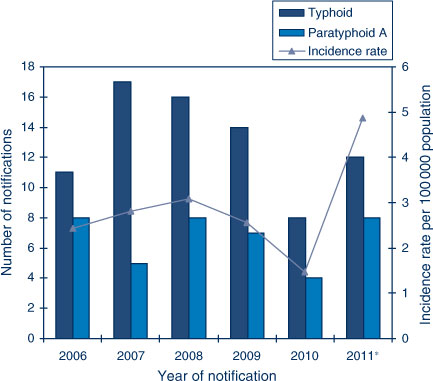
During the 5-year period 2006–2010, between 12 and 24 cases of enteric fever were reported in the Western Sydney Local Health District each year (rates per 100 000 population of 1.5–3.1) (Figure 1). However, in the 6 months from January–June 2011, 20 cases were reported, providing an estimated annual rate of 4.9 per 100 000 population. We investigated this higher-than-usual number of typhoid and paratyphoid cases in the Western Sydney Local Health District including describing the epidemiological, demographic and microbiological characteristics of these case-patients.
|
Methods
We undertook a retrospective, descriptive study of all confirmed cases of typhoid and paratyphoid A notified in the Western Sydney Local Health District between 1 January and 30 June 2011. Epidemiological, clinical and microbiological data were collated for each case-patient from public health unit, clinical and laboratory records. All age groups were included. A case of enteric fever was defined as the isolation of S. Typhi or S. Paratyphi from a sterile site or isolation from stool in a patient with the clinical features compatible with enteric fever. Serotyping was performed at the NSW Enteric Reference Laboratory, Institute for Clinical Pathology and Medical Research, according to the White-Kauffmann-Le Minor Scheme. Screening for reduced quinolone susceptibility was performed for isolates reported susceptible to ciprofloxacin, by testing nalidixic acid susceptibility using disc diffusion. This is an indicator of potential treatment failure if quinolone antibiotics are used for a patient.
Historical incidence data were extracted from the Notifiable Conditions Information Management System (NSW Health). Estimated resident populations in 2007 and 2010 were compiled by the Sydney West Epidemiology Unit from the census (Australian Bureau of Statistics).6 Ethics approval was not required as data collection was routine public health practice.
Results
Twenty culture-positive cases were notified to the public health unit overseeing the Western Sydney Local Health District between January and June 2011: 12 S. Typhi, and eight S. Paratyphi A. Nineteen isolates were from blood (plus stool in one instance) and one was from stool only. Three isolates showing ciprofloxacin susceptibility had reduced susceptibility or resistance to nalidixic acid (Table 1), thus full quinolone susceptibility was identified in only six isolates (one S. Typhi isolate from India, all three S. Typhi from Samoa, and two S. Paratyphi from India). Serotyping results from the three isolates that were acquired by case-patients in Samoa were the same (Table 1), suggesting a potential outbreak; two affected case-patients had attended the same large gathering and the third had attended a conference in Samoa.

|
Demographics
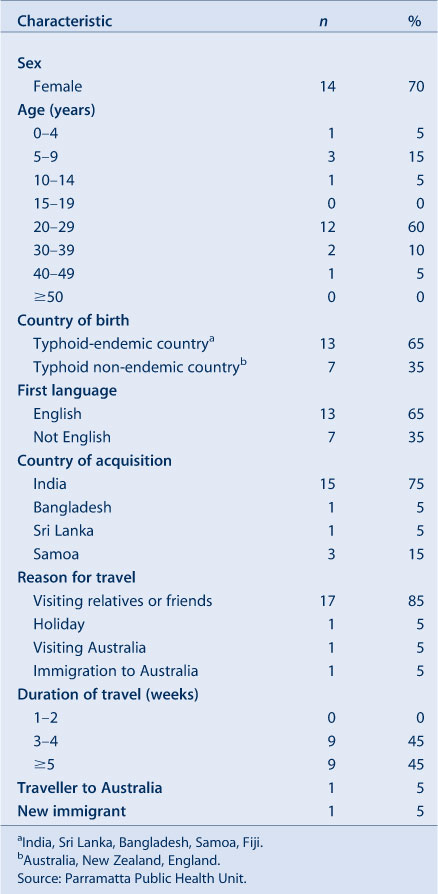
The median age of case-patients was 26 years (range 1–45 years) with the highest incidence in the 20–29-year age group (Table 2). Fourteen (70%) were females of whom two were pregnant. All but two were resident in Australia; of the two non-residents, one was a recent immigrant and the other a traveller from overseas.
|
Infection source
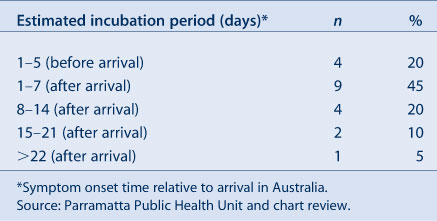
All case-patients had recently visited settings where typhoid is endemic (Table 3). The majority (n = 17) were travellers visiting family or friends. The median duration of travel was 28 days (range 21–70 days); no infections were reported in people who travelled for less than 3 weeks. Onset of illness was usually within 1 week of arrival in Australia (in one instance the interval was 23 days) (Table 4).
|
|
Signs and symptoms
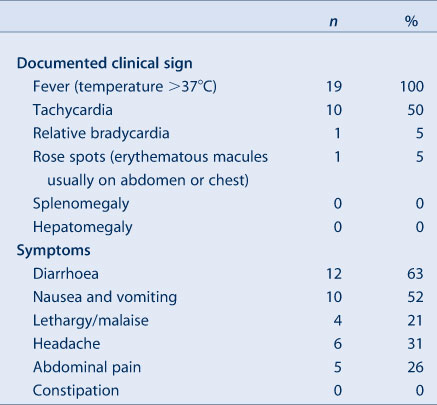
Of the 19 case-patients with a symptom history available, the most commonly reported symptom was diarrhoea (n = 12, 63%), followed by vomiting (52%), headache (31%), abdominal pain (26%) and lethargy (21%). None reported constipation. The most commonly reported clinical sign was fever. There were no serious complications and no deaths (Table 3).
Immunisation status
None of these 20 case-patients were immunised against typhoid. The reasons provided for lack of vaccination included, in one patient each, pregnancy, expense, being ‘too busy’ or thinking that the disease was too mild to warrant prevention.
Transmission-prone occupations
One patient was a chef who had a close contact working in farming. One was a community worker for disabled children and another was a teacher. These three patients were advised to refrain from working until their infection had been successfully cleared.
Discussion
This descriptive study provides a snapshot of recent enteric fever cases in the Western Sydney Local Health District of NSW. None of these case-patients had pre-travel vaccination and all infections were contracted outside Australia. In keeping with previous reports, these findings illustrate that migrants or people from non-English speaking backgrounds are at particular risk when they stay in typhoid-endemic areas for 3 weeks or more. Three case-patients were employed in potentially transmission-prone occupations, illustrating the importance of appropriate clinical questioning and public health action to prevent autochthonous transmission within Australia. There were no known instances of secondary enteric fever infections related to these cases.
Reasons for year-to-year variation in enteric fever numbers may reflect outbreaks in the countries visited or changing travel patterns. The possibility of an enteric fever outbreak in Samoa was suspected on the basis of three case-patients having attended large gatherings there and they were all infected with the same serotype. NSW Health officials contacted Samoan health authorities, however no increase in instances of enteric fever had been recognised locally. In another Pacific nation, Fiji, a ban was placed by government officials on public gatherings in the province of Bua in May 2011 due to an outbreak of typhoid.8
‘Visitors of friends and relatives’ (17 of these case-patients) are a recognised high-risk group for travel-acquired infections. They are less likely to seek pre-travel advice, more likely to engage in behaviours which increase likelihood of exposure to pathogens (e.g. staying with family in rural areas, drinking local water supplies), and often stay for longer periods.7,9 Improving pre-travel health advice to this at-risk group, in particular efforts to tailor pre-travel public health messages to Western Sydney Local Health District’s migrant population, could be effective in increasing the uptake of pre-travel vaccination and assist with preventing these diseases.
The costs to the health system associated with the care of these case-patients was considerable, with most requiring hospitalisation. In addition the individuals and their families experienced costs and distress. In comparison, the recommended retail cost of vaccination, excluding general practitioner fees, of both oral and parenteral preparations is less than $50; a combined hepatitis A and typhoid parenteral vaccine is also available.10,11 The relatively short duration of immunity (assumed as 3 years) from typhoid vaccine may be a deterrent to some people in vaccine uptake.
Young adults and school-aged children were the most affected, most likely reflecting the age of the travelling population. However, infrequent occurrence of confirmed cases in infants has also been demonstrated and attributed to the potential reluctance to obtain blood samples in infants,12,13 or to typhoid being milder or atypical in preschool years due to undeveloped reticuloendotheial systems.14 Infection is thought to confer at least partial protective immunity, which may account for lower rates in older travellers who were previously resident in endemic regions.15
Pregnant women were over-represented in this series. Pregnancy poses a particular risk for gastroenteric infections due to reduced gastrointestinal and biliary peristaltic activity and increased prevalence of biliary ‘sludge’ and concretions during pregnancy.16 Vaccination (with parenteral vaccine, as live oral formulations are contraindicated in pregnancy)4,5 is particularly recommended for pregnant women travelling to endemic areas because of their increased risk, and because of the relative contraindication to certain antimicrobial drugs during gestation.
Clinical features were mostly in keeping with previously published literature. Diarrhoea is a well-recognised symptom especially in the first week of illness, but the more classical picture is of constipation. Sixty-three percent of the patients in our series reported diarrhoea, exceeding rates of 6.5–25% reported elsewhere in immunocompetent people,1,17,18 perhaps due to their early stage of illness or reporting bias. One person experienced no abdominal symptoms, highlighting the importance of a high index of suspicion for this infection in returned travellers, and appropriate specimen collection. Rose spots were uncommon; these occur in 5–50% of enteric fever patients,1 however they are easily missed on people with dark skin and inexperienced clinicians may not recognise this sign. While no serious complications occurred in this group, relatively high complication rates of 10–15% are reported in endemic countries, possibly related to late presentation and under-reporting of milder cases.1
Most isolates showed reduced susceptibility or resistance to quinolone antibiotics, although all isolates from case-patients who acquired their infection in Samoa were fully sensitive. Knowledge of the geographical site of infection acquisition is helpful in determining empirical therapy. Current Australian guidelines recommend azithromycin as first-line therapy, or ceftriaxone if an intravenous agent is required, and still include the quinolone antibiotic, ciprofloxacin, as an alternative if infection was not acquired in the Indian subcontinent or South-East Asia.5,15 Our findings confirm the appropriateness of these recommendations.
This study was limited by its retrospective design, with potential for recall bias. Multiple physicians at different centres managed the patients, and notes were designed for medical purposes not audit, therefore the data were incomplete. While the numbers are small, they highlight issues relevant to efforts to improve prevention strategies.
Conclusion
Migrants returning to their home country may underestimate the risk of infection, and may require targeted public health pre-travel advice, especially if they intend to stay in a typhoid-endemic area for long periods. While there is no vaccine against paratyphoid fever, typhoid vaccination could have prevented up to 60% of these infections. Consequently travel health advice should be accessible and culturally appropriate.
Acknowledgments
We thank Peter Howard, NSW Enteric Reference Laboratory, Institute for Clinical Pathology and Medical Research (ICPMR), Westmead Hospital, for providing serotype results. APR is supported by a Sydney Medical School Foundation grant to the Sydney Emerging Infections and Biosecurity Institute, and NHMRC fellowship 1016567.
References
[1] Connor B, Schwartz E. Typhoid and paratyphoid in travellers. Lancet Infect Dis 2005; 5 623–8.| Typhoid and paratyphoid in travellers.Crossref | GoogleScholarGoogle Scholar |
[2] Crump JA, Luby SP. The global burden of typhoid fever. Bull World Health Organ 2004; 82 346–53.
[3] Kothari A, Pruthi A. The burden of Enteric fever. J Infect Developing Ctries 2008; 2 253–9.
[4] NSW Health. Typhoid Control Guideline, September 2004. Available at: http://www.health.nsw.gov.au/factsheets/guideline/typhoid.html (Cited 12 August 2011).
[5] Therapeutic Guidelines. Antibiotic, 14th edition. Melbourne: Therapeutic guidelines; 2010.
[6] Population Health and Strategic Direction. The Social Health Atlas. Sydney: Sydney West Area Health Service. Available at: http://westnet/services/dsdph_we/Epi/Publicat/Atlas3/index.htm (Cited 16 September 2011).
[7] Slinko VG, Jarvinen KA, Beard FH, McCall BJ. Notifications of enteric diseases in returning travellers who visit friends and relatives overseas: a call for action. Commun Dis Intell 2008; 32 333–4.
[8] ABC News. Fiji bans public gatherings after typhoid outbreak (Internet). 12 May 2011. Available at: http://www.abc.net.au/news/2011-05-12/fiji-bans-public-gatherings-after-typhoid-outbreak/2709844 (Cited 15 September 2011).
[9] Angell SY, Cetron MS. Health disparities among travellers visiting friends and relatives abroad. Ann Intern Med 2005; 142 67–72.
[10] MIMS online, via Clinical Information Access Portal. Available at: www.ciap.health.nsw.gov.au (Cited 22 June 2011).
[11] Yung A, Ruff T, Torresi J, Leder K, O’Briend D, eds. Manual of Travel Medicine: A pre-travel guide for health care practitioners. 2nd edition. Melbourne: IP Communications; 2004. pp. 276–7.
[12] Kidenya V, Ferson M. Typhoid and paratyphoid fever in south-eastern Sydney, 1992–1997. Commun Dis Intell 2000; 24 233–6.
[13] Siddiqui F, Rabbani F. Typhoid fever in children: some epidemiological considerations from Karachi, Pakistan. Int J Infect Dis 2006; 10 215–22.
| Typhoid fever in children: some epidemiological considerations from Karachi, Pakistan.Crossref | GoogleScholarGoogle Scholar |
[14] Mahle WT, Levine MM. Salmonella typhi infection in children younger than five years of age. Pediatr Infect Dis J 1993; 12 627–31.
| Salmonella typhi infection in children younger than five years of age.Crossref | GoogleScholarGoogle Scholar |
[15] Heyman DL, ed. Control of Communicable Diseases Manual 19th Edition. Washington DC: American Public Health Association; 2008.
[16] Touchan F, Hall JD, Lee RV. Typhoid fever during pregnancy: case report and review. Obstet Med 2009; 2 161–3.
| Typhoid fever during pregnancy: case report and review.Crossref | GoogleScholarGoogle Scholar |
[17] Clark TW, Daneshvar C. Enteric fever in a UK regional infectious diseases unit: a 10 year retrospective review. J Infect 2010; 60 91–8.
| Enteric fever in a UK regional infectious diseases unit: a 10 year retrospective review.Crossref | GoogleScholarGoogle Scholar |
[18] Patel T, Armstrong M. Imported enteric fever: case series from the hospital of tropical diseases, London, UK. Am J Trop Med Hyg 2010; 82 1121–6.
| Imported enteric fever: case series from the hospital of tropical diseases, London, UK.Crossref | GoogleScholarGoogle Scholar |