

9. Congenital conditions
NSW Public Health Bulletin 21(1) 93-101 https://doi.org/10.1071/NB10S09
Published: 24 June 2010
Congenital conditions among stillborn and live born infants
From 1 January 1998, doctors, hospitals and laboratories are required under the NSW Public Health Act 1991 to notify certain congenital conditions detected during pregnancy or in a baby up to 1 year of age. Information reported is included in the NSW Register of Congenital Conditions, formerly known as the NSW Birth Defects Register.
There are three types of conditions that are reported to the Register:
-
Conditions that affect the growth, development and health of the baby that are present before birth, such as cleft lip, dislocated hip and problems with the development of the heart, lungs or other organs
-
Conditions due to changes in the number of the baby’s chromosomes, such as Down syndrome
-
Four conditions due to changes in the baby’s inherited genetic information: cystic fibrosis, phenylketonuria, congenital hypothyroidism and thalassemia major.
Descriptions of some common congenital conditions are shown in Appendix 1. A list of common exclusions is shown in Appendix 2.
This chapter reports congenital conditions detected during pregnancy or in the first year of life for 2001–2006 and congenital conditions detected during pregnancy or at birth for 2007.
Trends in reported congenital conditions
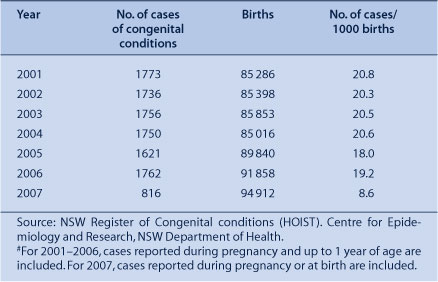
Between 2001 and 2004, the reported proportion of infants with congenital conditions has remained stable at about 2%, with a slight decline in 2005 and 2006 to 1.8 and 1.9%, respectively (Table 102). In 2007, 816 cases of congenital conditions detected during pregnancy or at birth were reported.
|
Congenital conditions by diagnostic category
The most common categories of congenital conditions for births of more than 20 weeks gestation or with a birth weight greater than 400 g are presented in Table 103. Congenital conditions are classified using the British Paediatric Association (BPA) Classification of Diseases, which is primarily organised by body system. For infants with more than one condition, each condition is counted separately. The number of congenital conditions reported therefore exceeds the number of affected infants.

|
In 2001–2007, conditions of the cardiovascular system were most commonly reported, followed by conditions of the musculoskeletal system and conditions of the genitourinary system (Table 103). This is a pattern similar to that in previous years. In 2006, the overall rate of conditions was similar to that in the previous 5 years (34.2 versus 34.6 per 1000, respectively).
Infant characteristics
In the period 2001–2007, a single condition was reported in 64.5% of infants, two conditions in 18.1%, three conditions in 7.9%, and four or more conditions in 9.5% of infants. The sex was male in 57.9% of infants, female in 41.7%, indeterminate in 0.3% of infants, and was not stated for 0.2%.
Congenital conditions were more common in preterm and post-term infants than in infants born at term (Table 104). Congenital conditions were also more common in infants born of a multiple pregnancy than a singleton pregnancy; in 2001–2007, 1.8% of singleton babies, 2.5% of twins, and 3.4% of triplets were born with a congenital condition.

|
About 11% of infants born with congenital conditions died in the perinatal period, over half of which were stillbirths (Table 105). These figures comprise all cases of congenital conditions, including those where the cause of death may not be directly related to the congenital condition(s). By comparison, the perinatal mortality rate among all births reported to the NSW Midwives Data Collection was less than 1% in 2007 (see Chapter 4).

|
Maternal characteristics
After 35 years of age, the incidence of congenital conditions increased with increasing maternal age (Table 106). Whereas the rate of congenital conditions is higher in older women, the majority of births occur in younger women. In 2001–2007, 74.2% of babies with congenital conditions were born to women aged less than 35 years.

|
In 2001–2007, 348 babies of Aboriginal or Torres Strait Islander mothers were reported to have congenital conditions. The rate of congenital conditions among these babies was 20.7 per 1000 compared with 17.2 per 1000 for babies born to non-Aboriginal mothers.
Congenital conditions among terminations of pregnancy, spontaneous abortions and unknown outcomes of pregnancy
The number of terminations of pregnancy reported to the Register increased from 257 in 2001 to 354 in 2006 (Table 107). In all, 178 terminations of pregnancy have been reported to the Register for 2007. This number is expected to increase as pregnancy outcomes for babies with conditions detected during pregnancy in 2007 continue to be reported.

|
Of the 1996 terminations of pregnancy reported in 2001–2007, 1555 (77.9%) were associated with a chromosomal anomaly, the most common of which was Trisomy 21 (Down syndrome), and 173 (8.7%) were associated with a neural tube defect (Table 108).

|
For spontaneous abortions, cytogenetic analysis is carried out only in cases of habitual abortion; the numbers presented, therefore, underestimate the number of spontaneous abortions that occur as a result of congenital conditions. Descriptions of some diagnostic terms used here are included in Appendix 1.
Trends in selected congenital conditions
Trends in a selection of common congenital conditions are shown in Table 109 and Figures 5–8. For 2001–2006, malformations reported up to 1 year of age are included. For 2007, malformations reported during pregnancy or at birth are included.

|
|
|
|
|
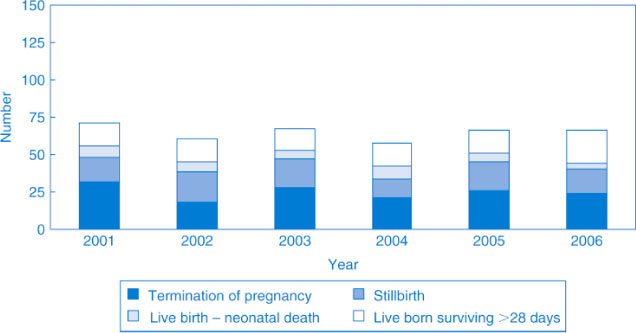
Over the period 2001–2006, the rate of neural tube defects has remained fairly stable at about 0.7 per 1000 births. The reported number of live born and stillborn infants with neural tube defects was 39 in 2001 and 42 in 2006, and 35 cases have been reported for 2007. The number of reported terminations of pregnancy was 32 in 2001, 24 in 2006, and 18 in 2007 (Figure 5).
Over the period 2001–2007, the number of cases of isolated cleft palate ranged from 52 to 90 per year, and for total cleft lip (including cases of cleft lip and cleft palate) from 58 to 88 per year. Termination of pregnancy was usually associated with other conditions such as neural tube conditions, chromosomal anomalies, or multiple anomalies in addition to the cleft lip and/or cleft palate.
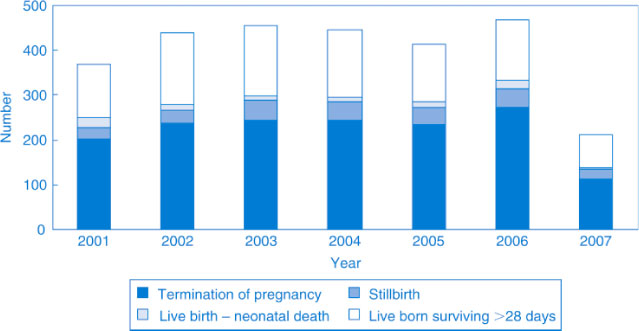
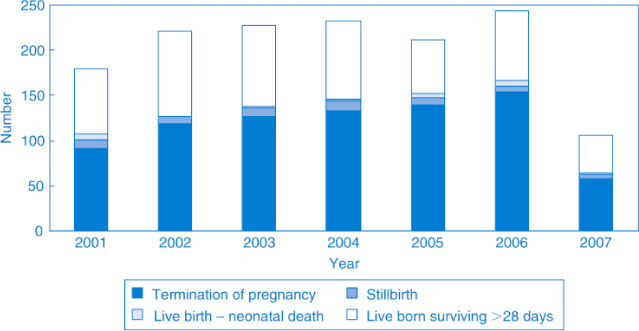
The reported number of live born and stillborn infants with chromosomal anomalies was 167 in 2001 and 195 in 2006. The number of reported terminations of pregnancy associated with chromosomal conditions rose from 202 in 2001 to 274 in 2006. The number of infants born with Down syndrome was 88 in 2001 and 90 in 2006, whereas the number of reported terminations of pregnancy associated with Down syndrome rose from 92 in 2001 to 154 in 2006 (Figure 7).
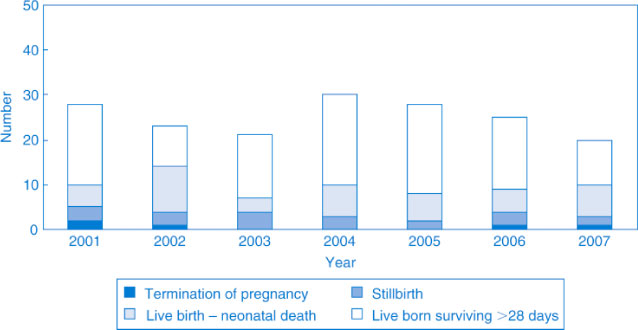
In 2001, 23 live born infants were reported to have a diaphragmatic hernia, three babies were stillborn and there were two terminations of pregnancy associated with this condition. In 2006, there were 21 live born infants reported with a diaphragmatic hernia, three stillborn babies and one termination of pregnancy (Figure 8).
Congenital conditions by NSW health areas
Crude rates of reported congenital conditions for NSW health areas and rates standardised for maternal age are shown in Table 110. The denominator population includes live births and stillbirths among NSW residents as reported to the MDC. The rate of congenital conditions increases with increasing maternal age (Table 106). To allow direct comparison of geographical areas, the rates have been standardised to the maternal-age distribution of births in NSW in 1991.

|
In interpreting congenital condition rates among NSW areas, it should also be noted that infants with congenital conditions who are born to mothers resident in areas close to interstate borders may be transferred interstate for care and therefore may not be reported to the Register.
Over the period 2001–2007, standardised rates of reported congenital conditions were lowest in the Greater Southern Area and highest in the Hunter and New England Area. Review of cases showed slightly increased reported rates of a wide range of congenital conditions in the Hunter and New England Area compared with NSW overall, including unstable hips (but not dislocated hips), talipes equinovarus, first-degree hypospadias, undescended testis, obstructive conditions of the renal pelvis and ureter, spina bifida, ventricular septal defect, atrial septal defect, patent ductus arteriosus, coarctation of the aorta and chromosomal anomalies. There was no clustering by small geographical area. The range and pattern of these conditions suggest that reporting of congenital abnormalities is better in the Hunter and New England Health Area than in NSW as a whole.