

Air quality and chronic disease: why action on climate change is also good for health
Martine Dennekamp A C and Marion Carey BA Monash Centre for Occupational and Environmental Health, Monash University
B Monash Sustainability Institute, Monash University
C Corresponding author. Email: martine.dennekamp@med.monash.edu.au
NSW Public Health Bulletin 21(6) 115-121 https://doi.org/10.1071/NB10026
Published: 16 July 2010
Abstract
There is increasing evidence that air pollution contributes to the burden of chronic disease and premature mortality, particularly from cardiovascular and respiratory causes. Action now urgently required to mitigate climate change has the potential co-benefit of improving air quality and reducing the chronic disease burden. Fossil fuel combustion, primarily from motor vehicles and energy generation, is a major contributor to anthropogenic climate change and air pollution-related health conditions. Action to reduce greenhouse gas emissions by improving energy efficiency, departing from carbon-intensive energy generation, facilitating mass transit and active transport options, also has the potential for significant public health benefits.
The first evidence of severe adverse health effects caused by ambient air pollution came from studies in the early twentieth century, which showed a relationship between episodes of extremely elevated concentrations of air pollution and elevated morbidity and mortality. The London smog episode of December 1952, which resulted in about 4000 excess deaths,1 led to the modern era of research into the effects of air pollution on human health. At present, a large body of evidence demonstrates that air pollution, even at concentrations below the current air quality standards, is associated with adverse health effects in humans.2–5 Climate change is expected to cause a decline in air quality.6 The good news is that action on climate change has the potential to reduce levels of air pollutants, resulting in significant public health benefits.
Air pollution is a complex chemical mixture whose effects on the individual can vary in time and place, making it difficult to differentiate between the effects of individual pollutants. The most common outdoor air pollutants in Australia that are relevant to health are: particulate matter (of varying size); ground-level ozone; oxides of nitrogen; carbon monoxide; and sulphur dioxide. There is an Australian Ambient Air Quality (AAQ) National Environment Protection Measure (NEPM) for many, but not all, of these pollutants. National Environment Protection Measures are legally binding standards for each level of government. Each jurisdiction is required to monitor and report performance in relation to the standards.
Particulate matter
Particulate matter (PM) includes airborne solid or liquid particles including dust, pollens, soot and aerosols from combustion activities. The most common measure of particulate air pollution is the routinely monitored PM10 (particles with a diameter less than 10 μm) in the ambient air. However in the past decade, interest has shifted towards the fine particle fraction of PM10, PM2.5 (particles with a diameter less than 2.5 μm), as particles of this size are able to penetrate deeper into the lungs and have the potential to be more damaging. In Australia, there is an air National Environment Protection Measure for PM10, however, unlike the United States of America (USA), there is only an advisory reporting standard for PM2.5. Advisory reporting standards do not have a time frame for compliance, and are used to gather data nationally to review the case for adoption of a compliance standard in the future.
Ozone
Ozone is a secondary pollutant formed, in the presence of sunlight, from the reaction of volatile organic compounds (emitted by the burning of fuels and evaporation from vegetation) and oxides of nitrogen (emitted by burning of fuels). Hot, dry weather conditions are conducive to ozone formation: it is sometimes called summer smog. Ozone is routinely monitored at ground level and has an enforceable National Environment Protection Measure.
This article will concentrate on ambient particulate matter and ozone as these are the most well researched air pollutants and their concentrations are most likely to be of increasing concern under climate change scenarios.6
How does air pollution contribute to chronic disease?
There is an extensive literature on the cardiorespiratory impacts of ambient air pollution, reporting a wide range of adverse health outcomes including exacerbation of chronic respiratory and cardiovascular disease, increased risk of cancer and premature mortality (Table 1).7,8

|
Sensitivity to the effects of air pollution differs according to individual susceptibility, age, and pre-existing health conditions. Young children, elderly people, those with chronic cardiac disease, and chronic respiratory disease such as asthma and chronic obstructive pulmonary disease, are generally more likely to be affected.9
There is good evidence that ambient air pollution can trigger the acute symptoms of, and exacerbate, both cardiac and respiratory disease. Recent evidence has supported a causal link between the development of asthma in children and exposure to traffic air pollution as well as the exacerbation of established asthma.8,10–12 However, at present there is insufficiently strong evidence to support a causal association for chronic disease in all instances.
Plausible biological mechanisms supported by experimental evidence exist whereby air pollution has the potential to cause cardiovascular disease,13 through, for example, contributing to a chronic inflammatory state increasing the risk of coronary atherosclerosis.14 However more population-based research is needed to confirm this hypothesis.
Particulate matter
Increased particle concentrations in ambient air have been associated with long-term effects on mortality as well as increased risks for admissions for cardiac and respiratory disease, including chronic obstructive pulmonary disease, pneumonia and ischaemic heart disease.15 In children particulate air pollution has been associated with increased chronic cough, and bronchitis.16 Globally, ambient PM air pollution has been estimated to be responsible for at least 0.8 million premature deaths and 6.4 million lost life years.17
Pope et al.18 in the USA found that each 10 μg/m3 elevation in ambient fine particulate air pollution was associated with approximately a 4%, 6% and 8% increased risk of all-cause, cardiopulmonary and lung cancer mortality, respectively. Chen and Goldberg19 reviewed 17 cohort studies and 20 case-control studies published 1950–2007 and found a 6% increase in non-accidental mortality for every increase of 10 μg/m3 in ambient fine particles, independent of age, gender and geographical regions. They then estimated that exposure to fine particles would lead to approximately 5000 deaths a year in Canada. Among these deaths, 1100 deaths would be from lung cancer and 2700 deaths would be from cardiovascular diseases. Kunzli et al.20 estimated the impact of total ambient air pollution on public health in Austria, France and Switzerland as a total mortality of 6%, or more than 40 000 attributable cases a year. About half of this pollution was attributed to motor vehicle traffic.
Ozone
Ozone exposure can cause lung inflammation resulting in decreased lung function and symptoms of respiratory irritation even in healthy people. It can also exacerbate bronchitis, emphysema and asthma.21 The effects of long-term ozone exposure have until recently not been clear, but they may contribute to chronic lung disease,21,22 and there is recent evidence of adverse effects on respiratory mortality.23
Australia
In Australia, significant associations have also been found between mortality and ambient air pollution.24,25 A study investigating the health effects of air pollution on daily mortality in Brisbane, Melbourne, Perth and Sydney found the strongest associations with particulate matter, nitrogen dioxide and ozone. For example, a 10 μg/m3 elevation in PM2.5 concentration was associated with approximately a 1% increase in the daily total number of deaths.26
Respiratory morbidity has been reported in association with outdoor air pollution in a number of Australian regions including the La Trobe Valley,27 the Newcastle and Wollongong areas of New South Wales (NSW)5 and the Melbourne region.28
What is the link between air quality and climate change?
Common sources of air pollutants and greenhouse gases
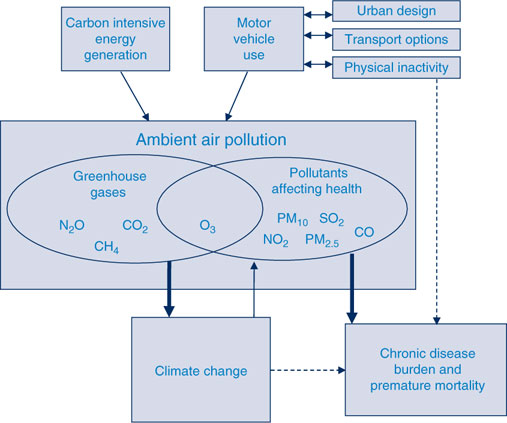
An important connection between climate change and ambient air quality is that greenhouse gas emissions which drive climate change, and the pollutants described earlier, frequently stem from common sources: primarily fossil-fuel combustion. The most important greenhouse gases emitted by carbon-intensive energy generation and motor vehicle use are carbon dioxide (CO2), methane (CH4) and nitrous oxide (N2O) (Figure 1). Ozone, also a greenhouse gas, can be formed near combustion sources, depending on the meteorological conditions. Fossil fuel combustion also results in the emission of the main ambient air pollutants affecting health which include particulate matter (PM2.5 and PM10), ozone (O3), sulphur dioxide (SO2), nitrogen dioxide (NO2) and carbon monoxide (CO) (Table 1).
|
Interconnection between meteorological variables and ambient air pollution levels
Greenhouse gases have an effect on climate which in turn has an effect on air pollutant levels,29 because factors like temperature, humidity, wind and precipitation can affect air pollutant emission, chemistry, deposition and transport.30 Climate change may enhance the adverse effects of ambient air pollutants due to chemical and physical interactions in the atmosphere. Adverse effects of ozone have been observed during the warmer seasons with evidence of synergistic effects between high temperature and ozone. Similar interactions between effects of ambient PM and temperature have been reported.31 Ozone in the troposphere can also act as a powerful greenhouse gas.
The interaction between increasing temperature and ambient air pollution in relation to health effects has also been found in Australia. For example, a study of temperature, air pollution and total mortality in summers in Sydney over the period 1994–2004 found that maximum temperature and sulphur dioxide air pollution had significant interactive effects on mortality.32 Temperature has also been found to modify the health effects of particulate matter in Brisbane.33 Furthermore, modelled effects of climate change in south eastern Australia predict that increasing bushfire risks will result in increasing levels of fine particles and volatile organic compounds.34
Emissions from transport sources
According to National Greenhouse Gas Inventory data for 2007, motor vehicle transport was responsible for 14.6% of greenhouse gas emissions in Australia.35 Transport emissions are also a major source of ambient air pollutants affecting health. A 2005 Australian Department of Transport working paper found motor vehicles were the principal source of nitrogen oxides and carbon monoxide in capital city airsheds (the geographical boundary for air quality standards), and that a high proportion of motor vehicle particulate emissions were very fine particles.36 The motor vehicle share of PM10 in capital city airsheds was 43% for Sydney, 31% for Brisbane, 33% for Melbourne, 19% for Adelaide, 20% for Perth and 10% for Hobart. The same study estimated that in the year 2000, motor-vehicle-related ambient air pollution accounted for between 900 and 2000 premature deaths in Australia.36
In Melbourne it is estimated that motor-vehicle emissions are responsible for 80% of the carbon monoxide, 60% of the nitrogen oxides, 40% of the volatile organic compounds and 30% of particulate matter in the outdoor air.37
Emissions from energy generating sources
In Australia 53.9% of greenhouse gas emissions come from stationary energy combustion (2007 data).35 Of the electricity generated in Australia, 81% is generated from coal, 13% from natural gas, 5% from hydro and 1% from other sources (including oil and wind).39 Electricity generation in Victoria, NSW region (includes the Australian Capital Territory) and Queensland is mainly fuelled by coal. In Western Australia, South Australia and the Northern Territory most electricity is generated by natural gas. Tasmania uses mostly hydrogeneration.39
Electricity generation and industrial production are major sources of PM2.5 and PM10 emissions in Australia, often more so outside capital city airsheds.38,40 For example, in the Sydney metropolitan airshed, industry contributes to 37% of PM10 emissions, but if the NSW Greater Metropolitan Region is considered (which includes the Newcastle and Wollongong regions as well as the greater Sydney region), 62% of PM10 emissions are from industry, primarily coal mining.40
Why would action to mitigate climate change help reduce the burden of chronic disease?
Policies that aim to reduce the rate of climate change by reducing greenhouse gas emissions are likely to produce a mutual benefit for health and the environment by reducing health-damaging ambient air pollutants and the related chronic cardiac and respiratory disease burden. While to date in Australia these two problems have been addressed by separate policies, to achieve the best outcome for climate and health, integrating them would be more effective.41
Figure 1 shows the interconnections between climate change, ambient air pollution and chronic disease. Action to mitigate climate change can potentially reduce the chronic disease burden because of decreasing air pollutant concentrations affecting health, increasing physical activity as an alternative to vehicle use42–44 and reducing the risk of other climate change-related impacts such as heatwaves, bushfires and dust storms.
Transport
Policies that aim to reduce motor vehicle use by increasing the use of alternative transport, and active transport such as walking and cycling, are also likely to reduce the risk of chronic non-communicable diseases such as obesity, cardiovascular disease and diabetes.45
Woodcock et al. used comparative risk assessment methods to estimate the benefits of alternative transport scenarios for London and Delhi, modelling health effects of ambient PM2.5.43 The scenario with the largest health gains for London (combined increased active travel and lower-emission motor vehicles) produced an estimated 10–19% reduction in the number of years-of-life lost from ischaemic heart disease, as well as reductions in cerebrovascular disease, depression, dementia and diabetes. This outcome did require large increases in distances walked and cycled and a 37% reduction in car use. The authors concluded that important health gains and reductions in CO2 emissions could be achieved through replacement of urban trips in private motor vehicles with active travel. However to achieve this level of health benefit, effective policies to increase distances walked and cycled and reduce car use are needed, with creation of safe and attractive urban environments for mass active travel.
Ozone standards have been exceeded every year since 1994 in the Sydney region, with levels sometimes reaching as much as double the standards.40 Since 1998, there has been no improvement in levels of ambient ground-level ozone in greater metropolitan Sydney.40 Despite improvements with fuel and vehicle emissions standards, the number of vehicles on the road has increased. Around a third of the car trips made in Sydney are less than 3 km and more than half are less than 5 km.34 Increasing the proportion of these short trips that are walked or cycled could have significant health and climate benefits.
Examples, such as the 1996 Olympic Games in Atlanta, illustrate what can be achieved relatively quickly. Traffic restrictions were put in place for the Games along with increased availability of alternative transport. During this time, peak daily ambient ozone concentrations decreased approximately 30% from baseline, which was associated with a significantly lower rate of asthma events.46
Energy generation
Modelling by Markandya et al.44 of changes in electricity production to reduce CO2 emissions with concomitant reductions in PM2.5 showed health gains in all countries studied, although gains were greatest in developing countries. Changes of modes of electricity generation were estimated to reduce not only carbon dioxide emissions but also particulate air pollution and consequently mortality. They predicted that by pursuing a climate target solely for electricity generation, 104 life-years per million people would be saved every year in the European Union (48 000 in total).
In Australia, major sources of pollution from energy generation and coal mining are often outside of capital city airsheds, e.g. Newcastle, Wollongong and the Latrobe Valley. However changes to these industries to reduce greenhouse gas emissions still have the potential to reduce the health impact on the local population.
Conclusions
Ambient air pollution is a significant contributor to both climate change and chronic disease. Effective policy needs to incorporate and understand the synergies between climate change and air pollution and the resulting health impacts. Moving away from carbon-intensive energy generation and motor vehicle dependence has the potential to reduce greenhouse gas emissions and the risk of harmful climate change. This action is necessary not only to reduce the range and severity of impacts from climate change, but also to reduce the morbidity and mortality that continues to be associated with poor air quality.
[1] Logan WPD, Glasg MD. Mortality in London fog incident, 1952. Lancet 1953; 261 336–8.
| Crossref | GoogleScholarGoogle Scholar | PubMed | (Accessed 1 March 2010.)
[35]
[36]
[37]
[38]
[39]
[40]
[41] Swart R, Amann M, Raers F, Tuinstra W. A good climate for clean air: linkages between climate change and air pollutants. Clim Change 2004; 66 263–9.
| Crossref | GoogleScholarGoogle Scholar | (Accessed 27 April 2010.)
[46] Friedman MS, Powell KE, Hutwagner L, LeRoy GM, Tegue WG. Impact of changes in transportation and commuting behaviours during the 1996 Summer Olympic Game in Atlanta on air quality and childhood asthma. JAMA 2001; 285 897–905.
| Crossref | GoogleScholarGoogle Scholar | PubMed | CAS |
