

Impact of policy changes of Medicare-rebated telehealth services on medical abortions provided at a family planning service during the coronavirus (COVID-19) pandemic
Yan Cheng A B , Clare J. Boerma A C , Kevin McGeechan A and Jane Estoesta A *
A B , Clare J. Boerma A C , Kevin McGeechan A and Jane Estoesta A *
A Family Planning NSW, 8 Holker Street, Newington, NSW 2127, Australia.
B Cancer Institute NSW, Level 4, 1 Reserved Road, St Leonards, NSW 2065, Australia.
C University of Sydney, 1-3 Ross Street (K06), NSW 2006, Australia.
Sexual Health 20(4) 357-359 https://doi.org/10.1071/SH22196
Submitted: 15 December 2022 Accepted: 15 June 2023 Published: 3 July 2023
© 2023 The Author(s) (or their employer(s)). Published by CSIRO Publishing
Abstract
This study reviewed data on the mode of delivery of medical abortion care (via face-to-face or telehealth) at a Family Planning service during the coronavirus (COVID-19) pandemic; April 2020 to March 2022. This was considered over time, in the context of changing eligibility criteria for Medicare-rebated telehealth services as well as patient demographic data. The study demonstrated that when Medicare rebates for telehealth are available for all those requiring abortion care, telehealth contributes to care provision alongside face-to-face services, and is more likely to be utilised by people living in regional and remote areas.
Keywords: epidemiology, family planning, primary care, public health, reproductive health, service delivery, social determinants, telehealth, women.
The coronavirus disease 2019 (COVID-19) pandemic has highlighted disparities in access to sexual and reproductive health (SRH) care, including access to abortion care globally and in Australia.1–3 In response to the pandemic, Medicare, Australia’s universal healthcare insurance scheme funded by Australian tax-payers, introduced nationwide rebates for telehealth in March 2020.4 This created new opportunities to provide abortion services via telehealth to complement existing face-to-face (F2F) services in Australia. Access to and information about abortion services in Australia varies across States and Territories. In New South Wales (NSW), one state in Australia, abortion was removed from the criminal code in October 2019. Medical abortion in Australian primary care requires prescription mifepristone and misoprostol to end a pregnancy before 9 weeks gestation. This can occur at home, with medical follow-up. In contrast, surgical abortion involves attendance at a surgical facility for vacuum curettage or dilation and evacuation of the uterine contents. Family Planning NSW (FPNSW), a statewide provider of SRH care, started offering abortion services in January 2020, following its decriminalisation in NSW, and then rapidly introduced telehealth (phone) medical abortion to complement F2F services in March 2020. However, in July 2020, primary care rebates were largely restricted to patients who had attended that service within the preceding year. This restriction was lifted for patients accessing SRH services from July 2021. Following our previous research letter which examined telehealth SRH care during the COVID-19 pandemic,5 this study investigated the trend in the number of patients accessing medical abortion via F2F and telehealth services at FPNSW during the periods with and without restriction in telehealth rebates, and compared characteristics of patients who used telehealth or F2F services to access medical abortion. The Family Planning NSW Ethics Committee provided ethics approval (R2020-04).
De-identified records for patients provided with Medicare-rebated medical abortion either via telehealth or a F2F consultation between 1 April 2020 and 31 March 2022 were extracted from the FPNSW clinical system. Data analysis was conducted to describe service provision and patient demographics over time. Analyses were conducted in SAS 9.4.
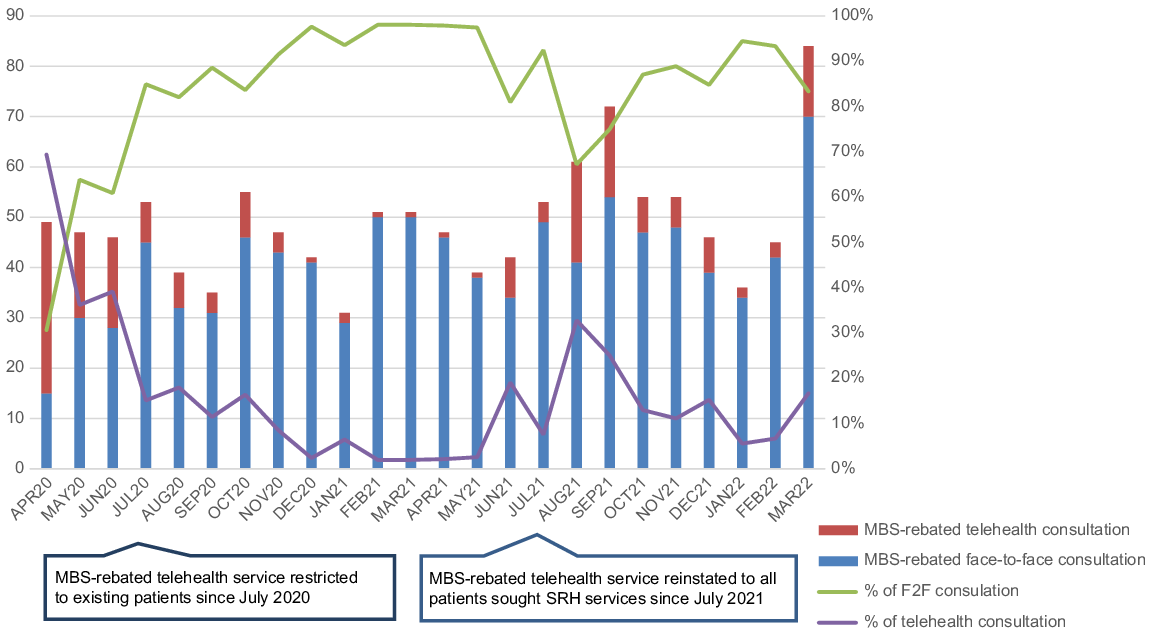
Of 1179 Medicare-rebated consultations providing medical abortion at FPNSW between 1 April 2020 and 31 March 2022, 197 (17%) used telehealth and 982 (83%) used F2F. Telehealth use was higher between April and June 2020 when the COVID-19 pandemic started in Australia, then decreased to a lower level between July 2020 and June 2021, when MBS-rebated telehealth services were restricted to existing patients. However, telehealth use increased between July 2021 and March 2022, when this restriction was removed for those seeking SRH care. In August 2022, the use of telehealth accounted for one-third of consultations providing medical abortion (Fig. 1).
Most of the demographics of patients using telehealth or F2F services were similar. However, patients who lived in regional and remote areas were more likely to use telehealth compared to patients who lived in major cities (59% and 21%, respectively for the period when MBS-rebated telehealth service restricted to existing patients between July 2020 and June 2021; and 42% and 20%, respectively, from July 2021 to August 2022).
Although F2F consultations remained the most popular model for abortion care, the availability of Medicare-rebated telehealth/phone services for all Medicare-eligible patients correlated with an increase in use of this mode of care clearly supported access to an essential SRH services during the COVID-19 pandemic. Access to abortion services can be difficult for women in rural and regional areas.6 Our findings support telehealth’s contribution in ensuring equitable access to medical abortion services.
References
1 Bateson DJ, Lohr PA, Norman WV, et al. The impact of COVID-19 on contraception and abortion care policy and practice: experiences from selected countries. BMJ Sex Reprod Health 2020; 46(4): 241-243.
| Crossref | Google Scholar |
2 Cousins S. COVID-19 has “devastating” effect on women and girls. Lancet 2020; 396(10247): 301-302.
| Crossref | Google Scholar |
3 Horan C, Palmer M, Shrestha R, Erlank CP, Church K. The impact of COVID-19 lockdown on abortion care: a time series analysis of data from Marie Stopes Nepal. Sex Reprod Health Matters 2022; 30(1): 2079185.
| Crossref | Google Scholar |
4 Australian Government Department of Health. COVID-19 temporary MBS telehealth services. 2022. Available at http://www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/Factsheet-TempBB
5 Cheng Y, Boerma C, Peck L, Botfield JR, Estoesta J, McGeechan K. Telehealth sexual and reproductive health care during the COVID-19 pandemic. Med J Aust 2021; 215(8): 371-372.
| Crossref | Google Scholar |
6 Subasinghe AK, McGeechan K, Moulton JE, Grzeskowiak LE, Mazza D. Early medical abortion services provided in Australian primary care. Med J Aust 2021; 215(8): 366-370.
| Crossref | Google Scholar |