

Frequency and extent of cognitive complaint following adult civilian mild traumatic brain injury: a systematic review and meta-analysis
Arielle M. Levy A , Michael M. Saling A and Jacqueline F. I. Anderson A B *
A , Michael M. Saling A and Jacqueline F. I. Anderson A B *
A Melbourne School of Psychological Sciences,
B Psychology Department,
Abstract
Cognitive symptoms are associated with return to work, healthcare use and quality of life after mild traumatic brain injury (mTBI). Additionally, while overall ‘post-concussion’ symptoms are often present at similar levels in mTBI and control groups, cognitive complaints may be specifically elevated in mTBI. A systematic review and meta-analysis was conducted to investigate the frequency and extent of cognitive complaints following adult civilian mTBI, and compare it to the frequency and extent of complaints in control populations (PROSPERO: CRD42020151284).
This review included studies published up to March 2022. Thirteen studies were included in the systematic review, and six were included in the meta-analysis. Data extraction and quality assessment were conducted by two independent reviewers.
Cognitive complaints are common after mTBI, although reported rates differed greatly across studies. Results suggested that mTBI groups report cognitive complaints to a significantly greater extent than control groups (Hedges’ g = 0.85, 95% CI 0.31–1.40, p = .0102). Heterogeneity between studies was high (τ2 = 0.20, 95% CI 0.04–1.58; I2 = 75.0%, 95% CI 43.4%–89.0%). Between-group differences in symptom reporting were most often found when healthy rather than injured controls were employed.
Cognitive complaints are consistently reported after mTBI, and are present at greater levels in mTBI patients than in controls. Despite the importance of these complaints, including in regards to return to work, healthcare use and quality of life, there has been limited research in this area, and heterogeneity in research methodology is common.
Keywords: mild traumatic brain injury, concussion, cognitive symptoms, cognitive complaints.
Mild traumatic brain injury (mTBI) is the most common type of traumatic brain injury, making up approximately 70%–90% of all traumatic brain injuries, and resulting in about 100-300/100,000 hospital-evaluated cases per year worldwide (Cassidy et al., 2004). Since many people with mTBI do not seek medical attention, researchers have estimated that the true prevalence of mTBI may be upwards of 600 people per 100,000 (Cassidy et al., 2004).
The prognosis following mTBI is considered to be largely positive, with reports suggesting that the majority of individuals recover fully within approximately 3 months (Carroll, Cassidy, Peloso, et al., 2004). Nevertheless, there is a subgroup of patients who experience poor recovery, evident by the reporting of ongoing ‘post-concussion’ symptoms. Recent research has suggested that this subgroup may be much larger than previously recognised, with potentially a majority of patients experiencing long-term post-concussion symptoms (Machamer et al., 2022).
Some of the most common self-reported post-concussion symptoms are cognitive symptoms, or cognitive complaints (Clarke et al., 2012). These refer to subjective reports of reduced cognitive ability, typically within the domains known to be affected in mTBI, including memory, attention, processing speed and executive function (Clarke et al., 2012; Ngwenya et al., 2018; Rabinowitz & Levin, 2014). Research suggests these symptoms can persist even several years following injury (Theadom et al., 2018), emphasising the need for further research in this area.
Cognitive complaints have received limited attention in mTBI research, possibly due to the fact that these symptoms do not reliably correspond to objective cognitive performance (Anderson, 2021; Stillman et al., 2019). In fact, research on cognitive performance suggests that the majority of individuals return to premorbid levels of cognitive functioning after mTBI (Iverson et al., 2019; Schneider et al., 2022). Nevertheless, cognitive symptoms continue to be reported, and these symptoms are associated with other important outcome factors after mTBI, including quality of life and return to work (Schraa, 1995; Theadom et al., 2017; Voormolen et al., 2019; Wrightson & Gronwall, 1981; Yousefzadeh-Chabok et al., 2021). In addition, cognitive symptoms are often the precipitant for referral to specialist neuropsychological services. Thus, it is important to understand these symptoms in order to improve patient outcomes, and to minimise the substantial financial burden of mTBI, of which healthcare use and delayed return to work are both large contributors (Te Ao et al., 2014). There is a paucity of research in this area, however, as most mTBI symptomatology research focuses only on overall post-concussion symptoms.
Cognitive symptoms are also particularly important because, in contrast to general post-concussion symptoms, cognitive complaints may differentiate between mTBI patients and control groups. There is a large body of research on the non-specificity of overall post-concussion symptoms, which are often found to be present at similar levels in mTBI patients and controls (Dean et al., 2012; Meares et al., 2011). There are intuitive reasons to expect that cognitive complaints, specifically, might be elevated in mTBI, and there is an assumption in clinical practice that this is the case. However, this assumption has not been formally assessed through prior review studies, and in actuality, cognitive symptoms are observed in a range of populations, including in non-brain-injured trauma patients and healthy individuals (Cargin et al., 2008; Iverson & Lange, 2003; Meares et al., 2011; Pullens et al., 2010). Thus, it is not currently clear whether these symptoms are greater (in frequency and/or severity) in patients with mTBI than in control populations, and further research is necessary to examine this hypothesis.
There are a number of factors to consider when exploring cognitive complaints after mTBI. Psychological factors (e.g. depression and anxiety) and female sex have consistently been linked to increased post-concussion symptoms after mTBI (Anderson & Jordan, 2021; Cnossen et al., 2018; Meares et al., 2006), and are therefore relevant, potentially confounding factors to consider in this area of research. Age is also known to affect symptoms after mTBI and is therefore another potential confound to consider (Cassidy, Boyle, et al., 2014; Hu et al., 2017; Li et al., 2017). Symptom reporting is also likely to be impacted by the duration after injury at which follow-up occurs (McCrea et al., 2009). Other considerations involve how mTBI is defined and how diagnosis is ascertained. Both of these factors determine the nature and representativeness of mTBI samples, and both commonly vary between studies and contribute to variability in study findings (Carroll, Cassidy, Holm, Kraus & Coronado, 2004).
This review is specifically interested in the patterns of cognitive complaints observed following civilian mTBI, as this represents the majority of mTBI. Civilians with mTBI represent a distinct subgroup in the mTBI literature as they experience different symptom burdens than individuals with military- or sports-related injuries (Beauchamp et al., 2021; Chapman & Diaz-Arrastia, 2014).
The aim of this systematic review and meta-analysis is to determine (1) the frequency and extent of cognitive complaints following adult civilian mTBI, and (2) whether these complaints are greater in mTBI relative to control groups. An additional aim is to review the quality of the existing literature on this topic.
Methods
Study protocol and search strategy
The protocol for this systematic review and meta-analysis was preregistered through PROSPERO (registration number: CRD42020151284). Reporting of this review followed Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines (Moher et al., 2009; Stroup et al., 2000).
The following databases were searched for studies published prior to 25 March 2022: Medline, PsycINFO, Emcare, Embase, Web of Science and Scopus. The full electronic search strategy is given in the Appendix (see Supplementary Material).
Inclusion and exclusion criteria
Studies of interest for inclusion in the systematic review were peer-reviewed journal articles reporting cognitive complaint data following adult civilian mTBI. Studies were eligible for inclusion whether they reported this data as frequency data (e.g. the proportion of a sample reporting cognitive complaints) or as continuous data (e.g. scores on a cognitive complaint scale). Note that continuous data was interpreted as representing the overall extent of cognitive complaint, as higher scores on each scale could indicate either a greater number of symptoms endorsed, symptoms endorsed to a greater severity or both. Studies were also eligible whether or not they included a control group. The complete list of inclusion and exclusion criteria is listed in Table 1.
Inclusion and exclusion criteria for each study
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
|
|
Study screening, data extraction and quality analysis
Covidence online systematic review software (Veritas Health Innovation, 2019) was used for study screening, data extraction and quality analysis. The first author conducted title and abstract screening and full-text screening. Studies that passed full-text screening were reviewed with the final author for consensus for inclusion in the review.
Two independent reviewers completed data extraction and quality analysis for each included study. Any disagreements were settled through discussion until consensus was reached. Where the two primary reviewers could not reach consensus, a third reviewer was engaged and majority opinion was taken. Data extracted from each study included study design data, participant characteristics and demographics, and cognitive symptom data. Study authors were contacted for numerical data values in cases where symptom data was reported in figures.
The quality of each study was evaluated using the Newcastle–Ottawa Scale (NOS), designed to assess the quality of non-randomised studies included in systematic reviews (Wells et al., 2000). The NOS is recommended by the Cochrane Collaboration as well as various methodological review papers (Deeks et al., 2003; Higgins & Green, 2011; Zeng et al., 2015). The cohort study version of this scale evaluates studies on the domains of group selection, comparability of study groups and ascertainment of outcome. Studies are eligible for a maximum of one ‘star’ for each item within the selection and outcome categories, and a maximum of two stars for the comparability item. The form was modified to fit the current research question. As several included studies were case series and did not include a control group, the scale was additionally modified for use with these studies, similar to previous approaches (Lawley et al., 2015; Murad, Sultan, Haffar & Bazerbachi, 2018).
Data analysis
Intended analyses included determining the overall frequency of cognitive complaints, subgroup analyses examining cognitive domain and time since injury, and comparison of the extent of cognitive complaints in mTBI and control groups. Due to their non-comparability, frequency data and continuous data were analysed separately.
The summary measure used for meta-analysis was the standardised mean difference (SMD). The SMD is a measure of effect size that allows for pooling of outcome data across the use of different outcome scales through standardising the difference between groups in each study. The current meta-analysis used Hedges’ g, a specific form of SMD, which corrects for bias in effect size estimations when small samples are used (Borenstein et al., 2009).
A random-effects model was used to pool outcomes, based on the expectation that included studies would differ in their underlying true effects, a scenario that is highly likely due to methodological differences in studies being combined (Borenstein et al., 2009). The Hartung–Knapp adjustment was applied to the model to reduce the risk of a false positive result, which meta-analyses can be particularly susceptible to when they contain a small number of studies with substantial heterogeneity (Inthout, Ioannidis & Borm, 2014).
Heterogeneity between studies was quantified using τ2 and I2. τ2 is defined as the variance of the true effect sizes of the population of studies, on the same scale as the SMD. Thus, on a distribution of the true underlying effect sizes, the SMD is the estimate of the mean of the distribution, and τ2 is the variance of the distribution (Borenstein et al., 2009). To estimate τ2, the restricted maximum-likelihood method was used, as recommended by Veroniki et al. (2016). I2 gives the percentage of the total observed variation that is attributed to differences in true effect sizes underlying the included studies, as opposed to random error (where total variation can be thought of as the sum of the true between-studies variation and the within-study error) (Borenstein et al., 2009). I2 can range from 0% to 100% and I2 values of 25%, 50% and 75% can be interpreted as indicating low, moderate and high heterogeneity, respectively (Higgins, Thompson, Deeks & Altman, 2003).
All quantitative analysis was conducted in R (version 3.6.1; R Development Core Team, 2011) using the following packages: tidyverse (Wickham et al., 2019), meta (Balduzzi, Rücker & Schwarzer, 2019) and dmetar (Harrer, Cuijpers, Furukawa & Ebert, 2019).
Results
As shown in Fig. 1, 3057 studies were screened by the first author for inclusion in the systematic review, of which 445 were assessed through full-text review. The resulting 19 papers underwent review by the first and last author, with a further 6 papers excluded by consensus (see Fig. 1 for exclusion reasons). The 13 remaining papers were included in the systematic review (Anderson, 2021; Clarke, Genat & Anderson, 2012; Hou et al., 2012; Landre et al., 2006; Marsh & Smith, 1995; Mayer et al., 2015; Norman, Shah & Turkstra, 2019; Pacella, Prabhu, Morley, Huang & Suffoletto, 2018; Raz et al., 2011; Shumskaya, Andriessen, Norris & Vos, 2012; Studerus-Germann et al., 2017; Stulemeijer, Vos, Bleijenberg & van der Werf, 2007; Sullivan et al., 2017).
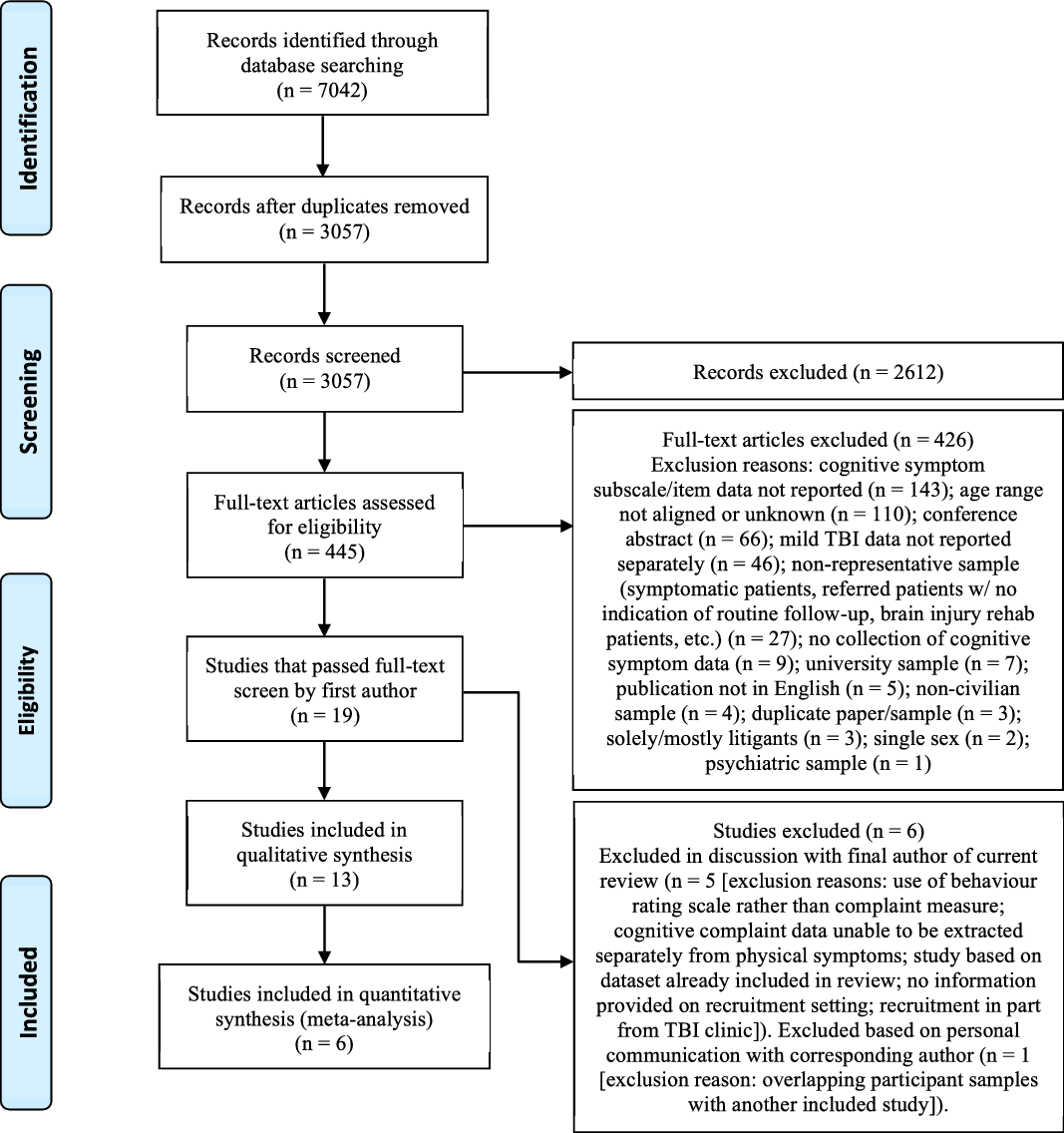
One of the most common reasons for exclusion during full-text review was on the basis of age range of participants. Importantly, this was often due to insufficient reporting of information, as approximately one quarter of the studies excluded on this basis did not report participant age range.
Of the 13 included papers, study authors were contacted for numerical data values in the case of four studies where outcome data was reported in figures (Hou et al., 2012; Pacella et al., 2018; Studerus-Germann et al., 2017; Stulemeijer et al., 2007). This additional data was provided for one study (Studerus-Germann et al., 2017). For the remaining studies, figures reporting cognitive complaint data were used to derive ranges of symptom endorsement. These data ranges were included in the qualitative synthesis but were not included in the meta-analysis.
Systematic review
There was 83.33% agreement between raters across the three NOS domains. Inter-rater reliability yielded a Cohen’s kappa of 0.73. This reflects moderate agreement by conservative approaches, and is high relative to previous research using the same scale (Hartling et al., 2012; McHugh, 2012).
Table 2 presents ratings on the modified NOS scale for each included study. The total number of stars that each study was eligible for varied due to variability in study design. Only four of the 13 included studies were awarded a star on 80% or more of the eligible items (Clarke et al., 2012; Hou et al., 2012; Landre et al., 2006; Raz et al., 2011).
Star ratings on the modified NOS scale for each included study
| Anderson (2021) | Clarke et al. (2012) | Hou et al. (2012) | Landre et al. (2006) | Marsh & Smith (1995) | Mayer et al. (2015) | Norman et al. (2019) | Pacella et al. (2018) | Raz et al. (2011) | Shumskaya et al. (2012) | Studerus-Germann et al. (2017) | Stulemeijer et al. (2007) | Sullivan et al. (2017) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of exposed (mTBI) cohort | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | |
| Selection of non-exposed cohorta | – | ★ | ★ | – | ★ | ★ | – | |||||||
| Ascertainment of mTBI exposure | ★ | ★ | ★ | ★ | – | – | ★ | ★ | ★ | – | ★ | – | – | |
| Comparability of cohortsa | ★ | ★ | ★ | ★★ | – | ★ | ★ | |||||||
| Follow-up length sufficient for outcomes to occur? | ★ | ★ | ★ | ★ | ★ | ★ | ★ | – | ★ | ★ | ★ | ★ | ★ | |
| Adequacy of cohort follow-upa | ★ | – | – | – | – | |||||||||
| # of stars out of total eligible | 4/6 | 5/6 | 4/4 | 5/6 | 2/4 | 4/6 | 4/6 | 4/7 | 3/3 | 3/6 | 3/4 | 2/4 | 2/3 | |
| % of stars out of total eligible | 67% | 83% | 100% | 83% | 50% | 67% | 67% | 57% | 100% | 50% | 75% | 50% | 33% |
Each study was deemed to have a sample that was sufficiently representative of adult civilian mTBI, which was expected given that this was an inclusion criterion for the review. Additionally, almost all studies were considered to have employed a follow-up length sufficient for outcomes to occur, defined as follow-up ≥24 h after injury. However, there were some methodological shortcomings in other areas assessed by the NOS scale. Where follow-up was present, nearly all studies either had insufficient follow-up rates – defined as rates <80% (Marsh & Smith, 1995; Pacella et al., 2018; Studerus-Germann et al., 2017) – or failed to provide this information (Stulemeijer et al., 2007). Studies were also likely to introduce potential bias through failing to ensure comparability of mTBI and control cohorts by not controlling for sex (Landre et al., 2006; Norman et al., 2019) or psychological factors (Clarke et al., 2012; Norman et al., 2019; Pacella et al., 2018; Shumskaya et al., 2012).
The characteristics of included studies are listed in Table 3. The sample size of each study ranged from 15 mTBI participants to 107 mTBI participants. Across the included studies, there were a total of 546 mTBI participants with cognitive complaint data available.
Characteristics of studies included in systematic review
| Studya | Study type | mTBI recruitment details | Control group typeb | nc | Sample aged | Sex (% female) | Follow-up time post-injurye | Scale | Type of data reported | Format of reported data | Findingsf | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [Mean (SD), Range] | ||||||||||||
| Anderson (2021) | Prospective | Patients admitted to hospital | HC | mTBI: 52 | mTBI: 35.75 (14.70), 18–60; | mTBI: 21% | 6–12 weeks | CCAMCHI | Scale total | Means, SDs | Average total scores were 94.09 (SD = 7.33) for the mTBI group and 85.34 (SD = 7.70) for the HC group. The difference between groups was significant (p = .002) | |
| HC: 57 | HC: 31.04 (11.11), 18–56 | HC: 65% | ||||||||||
| Clarke et al. (2012) | Prospective | Patients admitted to neurosurgery unit of hospital | SI; HC | mTBI: 21 | mTBI: 35.6, 19–60 | mTBI: 33% | 3–12 months | PACCQ | Scale total | Means, SDs | Average total scores were 96.90 (SD = 8.20) for the mTBI group, 92.53 (SD = 3.64) for the SI group and 88.20 (SD = 10.84) for the HC group. The difference between the mTBI and HC groups was significant (mean difference = 8.70, SE = 2.56, p = 0.004) | |
| SI: 19 | SI: 34.1, 18–58 | SI: 26% | ||||||||||
| HC: 20 | HC: 19.0, 18–28 | HC: 40% | ||||||||||
| Hou et al. (2012) | Prospective, longitudinal | Patients presenting to hospital ED | N/A | 107 | 38.32 (14.14)g, 18–60 | 37% | 3 months; 6 months | RPQ | Item data (Forgetfulness, poor memory; poor concentration; taking longer to think) | Frequencies | ‘Forgetfulness, poor memory’ was endorsed by 25–30% of the sample at 3 months and 15–20% of the sample at 6 months. Poor concentration was endorsed by 15–25% of the sample at 3 months and 15–20% at 6 months. Taking longer to think was endorsed by 20–25% of the sample at 3 months and 15–20% at 6 months | |
| Landre et al. (2006) | Prospective | Patients admitted to hospital trauma department | TC | mTBI: 37 | 18–60 | mTBI: 38% | mTBI: 3.87 ± 4.40 days; TC: 5.08 ± 5.47 days | Modified version of PCSC | Scale subscore | Means, SDs | Mean total scores on the cognitive subscale was 12.51 (SD = 5.00) for the mTBI group and 11.38 (SD = 4.29) for the TC group. The difference between groups was not significant | |
| mTBI: 33.11 (9.97); | ||||||||||||
| TC: 39 | TC: 36.46 (11.20) | TC: 26% | ||||||||||
| Marsh & Smith (1995) | Prospective, longitudinal | Patients “treated for concussion” at hospital | N/A | 15 (n = 11 for first follow-up) | 27.07 (12.60), 18–56 | 20% | 2 weeks; 1 month; 3 months | CFQ | Scale total | Means, SDs | Mean total scores were 46.27 (SD = 22.81), 39.67 (SD = 19.66) and 28.93 (SD = 14.93) at 2 weeks, 1 month and 3 months, respectively | |
| Mayer et al. (2015) | Prospective | Recruitment setting not specified | HC | mTBI: 46 | 18–55 | mTBI: 48% | 13.7 ± 5.0 days | NSI | Scale subscore | Means, SDs | The average total subscale score was 4.7 (SD = 3.4) for the mTBI group and 1.4 (SD = 2.3) for the HC group. This difference was significant (F1,89 = 28.53, p < 0.001, d = 1.12) | |
| mTBI: 28.9 (9.8) | ||||||||||||
| HC: 46 | HC: 28.4 (9.9) | HC: 48% | ||||||||||
| Norman et al. (2019) | Prospective | Patients presenting to hospital ED | OI | mTBI: 20 | mTBI: 29.20 (10.77), 19.6–52; | mTBI: 57% | 3–12 weeks | NSI | Scale subscore | Means, SDs | The average total subscale score was 3.75 (SD = 2.83) for the mTBI group and 2.76 (SD = 3.25) for the OI group. This difference was not significant | |
| OI: 21 | OI: 28.23 (7.58), 18.5–48 | OI: 73% | ||||||||||
| Pacella et al. (2018) | Prospective, longitudinal | Patients presenting to hospital ED | HI (i.e. injury to the head without mTBI); TC | mTBI: 39 | 18–55 | mTBI: 49% | 1–14 days | RPQ; RPQ-based experience sampling questions | Item data (Concentration difficulty) | Frequencies | In the mTBI group, 40–60% experienced concentration difficulties every day, and 0–20% did not experience concentration difficulties on any day. In the TC group, 20–40% experienced concentration difficulties every day, and 20–40% of the group did not experience any concentration difficulties. No differences were detected between the mTBI group and HI group. The odds difference in symptom reporting between the mTBI and TC groups became non-significant by day 8 post-injury. Pre-injury concentration difficulties were reported by 36%, 25% and 28% of the mTBI, HI and TC groups, respectively. | |
| mTBI: 32 (12.1) | ||||||||||||
| HI: 16 | HI: 36 (9.9) | HI: 50% | ||||||||||
| TC: 53 | TC: 34 (11.1) | TC: 45% | ||||||||||
| Raz et al. (2011) | Prospective | Recruited from hospital records and ED | N/A | 28 | 35.6 (10.4), 18–60 | 32% | MRI 559 ± 803 days; symptom data within 24 h of MRI | PCSS | Item data (Memory loss) | Frequencies | 8 patients (29% of sample) reported experiencing memory loss | |
| Shumskaya et al. (2012) | Prospective | Patients admitted to hospital ED | HC | mTBI: 32 | mTBI: 39, 18–60h | mTBI: 37%h | 2–28 days (mean = 9 days) | RPQ | Scale subscore | Means, IQR, score range | The average cognitive score for the mTBI group was 25.0 (IQR = 24.3; range 0–75) and the average cognitive score for the HC group was 0.0 (IQR = 16.3; range 0–50). The difference between groups was significant (p = 0.010). | |
| HC: 32 | HC: 38, 19–59h | TC: 37%h | ||||||||||
| Studerus-Germann et al. (2017) | Prospective | Patients presenting to hospital ED | N/A | 23 | 35.0, 18–55i | 47%i | 3 months | ImPACT PCSS | Item data (Difficulty concentrating, difficulty remembering, feeling slowed down, feeling mentally “foggy”) | Means | Mean scores on the rating scale were as follows, for the 3-day and 7-day return to work groups, respectively: 1.45 and 0.75 (‘difficulty concentrating’); 1.09 and 1.25 (‘difficulty remembering’), 0.55 and 0.25 (‘feeling slowed down’); and, 0 and 0 (‘feeling mentally “foggy”’).j Note: participants did not follow the return to work recommendations; the 3-day group returned to work later than the 7-day group on average | |
| Stulemeijer et al. (2007) | Prospective, longitudinal | Patients presenting to hospital ED | N/A | 79 | 18–60 | 38% | 6 months (longitudinal follow-up over 12 days) | RPQ; SOL | Scale subscore [RPQ]; Item data [SOL] (memory problems, concentration problems) | Frequencies | 39% of sample reported ‘serious’ CCs. No difference was found in diary ratings of cognitive problems between groups; memory problems were experienced 10% and 9% of the time in these groups, respectively, and concentration problems were experienced 11% and 6% of the time, respectively. Memory and concentration problems were highest around the middle of the day and lowest at the start and end of the day | |
| CCs: 37.7 (13.5) | ||||||||||||
| No CCs: 36.8 (12.3) | ||||||||||||
| Sullivan et al. (2017) | Prospective | Patients admitted to ED of tertiary-referral hospital | N/A | 38 | 34.71 (11.81), 18–60 | 42% | 11.5 ± 6.49 days (median: 10.5, range: 2–33) | NSI | Scale subscore | Means, SDs | The mean response on the cognitive items was 0.52 (SD = 0.90), and the average total score for these items was 2.07 (SD = 3.61) |
CC, cognitive complaint; CCAMCHI, Cognitive Complaint After Mild Closed Head Injury; CFQ, Cognitive Failures Questionnaire; ED, emergency department; HC, healthy control; HI, head injury; ImPACT PCSS, Immediate Post-Concussion Assessment and Cognitive Test post-concussion symptom scale; IQR, interquartile range; MRI, magnetic resonance imaging; NSI, Neurobehavioral Symptom Inventory; OI, orthopedic injury; PCSC, Post-concussive Symptom Checklist, PACCQ, Post-Hospital Admission Cognitive Complaint Questionnaire; RPQ, Rivermead Post-Concussion Symptoms Questionnaire; SD, standard deviation; SI, spinal injury; SOL, Self-Observation List; TC, trauma control
The features required for diagnosis of mTBI differed greatly between included studies, despite many studies basing their criteria on the same published definitions of mTBI. A comparison of mTBI definition between studies is shown in Table 4. This table highlights the variation in definitions of mTBI across studies. Note that if study definitions were equivalent, each column of the table would be identical.
Definition of mTBI in studies included in systematic review
| Key features of definition | Anderson (2021) | Clarke et al. (2012) | Hou et al. (2012) | Landre et al. (2006) | Marsh & Smith (1995) | Mayer et al. (2015) | Norman et al. (2019) | Pacella et al. (2018) | Raz et al. (2011) | Shumskaya et al. (2012) | Studerus-Germann et al. (2017) | Stulemeijer et al. (2007) | Sullivan et al. (2017) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alteration in mental state | (✓) | (✓) | (✓) | ✓ | (✓) | (✓) | ✓ | |||||||
| Loss of consciousness: | ||||||||||||||
| ≤15 mins | (✓) | |||||||||||||
| ≤20 mins | (✓) | |||||||||||||
| <30 mins | (✓) | (✓) | ||||||||||||
| ≤30 mins | (✓) | ✓ | (✓) | (✓) | (✓) | ✓ | (✓) | |||||||
| 1–30 mins | (✓) | |||||||||||||
| Any duration | (✓) | |||||||||||||
| Post-traumatic amnesia: | ||||||||||||||
| ≤60 mins | (✓) | |||||||||||||
| <60 mins | (✓) | |||||||||||||
| <24 h | (✓) | (✓) | ||||||||||||
| ≤24 h | ✓ | (✓) | (✓) | (✓) | ✓ | (✓) | ||||||||
| Any duration | (✓) | |||||||||||||
| GCS Score: | ||||||||||||||
| 13–15 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | (✓) | |||
| 15 | ✓ | |||||||||||||
| CT findings: | ||||||||||||||
| Present | ||||||||||||||
| Absent | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Focal neurological deficit(s): | ||||||||||||||
| Present | (✓) | (✓) | ||||||||||||
| Absent | ✓ | ✓ | ||||||||||||
| Skull fracture/penetrating injury: | ||||||||||||||
| Present | (✓) | |||||||||||||
| Absent | ✓ | ✓ | ✓ | |||||||||||
| Published mTBI definition referenced? | WHO | – | ACRM | ACRM | – | – | ICD9 Codes 850, ICD10 Codes S06.0 | ACRM | ACRM | – | – | EFNS | WHO |
Note. A standard checkmark indicates required features, and a checkmark in brackets indicates features that were considered in the definition but not specifically required (i.e. optional features, or situations in which only one of a set of features was required). Some definitions were unclear; this represents best interpretation. For studies where comprehensive diagnostic information was not provided (Norman et al., 2019; Stulemeijer et al., 2007), additional information was obtained from published definitions cited within these studies (Eisenberg et al., 2014; Vos et al., 2002). The variation both in features of the definition (represented by each row) and whether the feature was required (represented by each symbol) highlights the degree of heterogeneity in definitions of mTBI across studies.
ACRM, American Congress of Rehabilitation Medicine; EFNS, European Federation of Neurological Societies; GCS, Glasgow Coma Scale; ICD, International Classification of Diseases; WHO, World Health Organization
Ten of the 13 studies included a control group, but only seven had control groups within the required age range of this review (i.e. age 18–60) and with cognitive complaint data available. Of these studies, three employed healthy controls (Anderson, 2021; Mayer et al., 2015; Shumskaya et al., 2012), three employed injured controls (Landre et al., 2006; Norman et al., 2019; Pacella et al., 2018) and one employed both (Clarke et al., 2012). One study also employed a ‘head injury’ group of trauma patients who sustained an injury to the head but did not meet criteria for mTBI (Pacella et al., 2018). Across these studies, there were a total of 148 injured controls and 155 healthy controls with cognitive complaint data available.
Follow-up times within included studies ranged from approximately 1 day post-injury (Pacella et al., 2018) to approximately 1.5 years post-injury (Raz et al., 2011). Six studies collected cognitive complaint data at or within an average of 2 weeks post-injury (Landre et al., 2006; Marsh & Smith, 1995; Mayer et al., 2015; Pacella et al., 2018; Shumskaya et al., 2012; Sullivan et al., 2017), three studies collected this data between 2 weeks and 3 months post-injury (Anderson, 2021; Marsh & Smith, 1995; Norman et al., 2019), five studies collected this data at or between 3 and 12 months post-injury (Clarke et al., 2012; Hou et al., 2012; Marsh & Smith, 1995; Studerus-Germann et al., 2017; Stulemeijer et al., 2007) and one study collected this data at more than 1 year post-injury (Raz et al., 2011). Four studies reported cognitive complaint data at multiple time-points (Hou et al., 2012; Marsh & Smith, 1995; Pacella et al., 2018; Stulemeijer et al., 2007).
Most studies reported continuous outcome data rather than frequency data. This was either in the form of mean total scores on a scale of cognitive complaints (n = 3; Anderson, 2021; Clarke et al., 2012; Marsh & Smith, 1995) or mean cognitive subscores on a scale of post-concussive symptoms (n = 6; Landre et al., 2006; Mayer et al., 2015; Norman et al., 2019; Shumskaya et al., 2012; Studerus-Germann et al., 2017; Sullivan et al., 2017). The specific cognitive functions assessed by each scale are listed in Table 5.
Cognitive functions assessed by each scale
| Targeted cognitive complaint scalesa | |
|---|---|
| Cognitive Failures Questionnaire (CFQ) | |
| Perception | |
| Memory | |
| Motor function | |
| Post-Hospital Admission Cognitive Complaint Questionnaire (PACCQ) and Cognitive Complaint After Mild Closed Head Injury (CCAMCHI)b | |
| Memory | |
| Attention | |
| Processing speed | |
| Executive function | |
| Post-concussion symptom scalesc | |
| Rivermead Post-concussive Symptoms Questionnaire (RPQ) | |
| Forgetfulness, poor memory | |
| Poor concentration | |
| Taking longer to think | |
| ImPACT Post-Concussion Symptoms Scale (PCSS) | |
| Difficulty remembering | |
| Difficulty concentrating | |
| Feeling slowed down | |
| Feeling like you are ‘in a fog’ | |
| Neurobehavioral Symptom Inventory (NSI) | |
| Forgetfulness | |
| Poor concentration | |
| Difficulty making decisions | |
| Slowed thinking | |
| Modified Post-Concussion Syndrome Checklist (PCSC) | |
| Memory problems | |
| Trouble concentrating | |
| Difficulty finding words when speaking |
In contrast to the studies reporting continuous outcome data, four studies reported dichotomous outcome data (Hou et al., 2012; Pacella et al., 2018; Raz et al., 2011; Stulemeijer et al., 2007), that is, frequencies or percentages of the sample endorsing cognitive complaints.
One study looked at the overall prevalence of cognitive complaints (Stulemeijer et al., 2007). This study found that 39% of their sample reported ‘serious’ cognitive complaints, defined as scores on a cognitive subscale that fell two or more standard deviations above the mean of an injured control group.
With respect to overall cognitive symptoms over time, one study found that subjective cognitive symptoms decreased significantly from 2 weeks to 1 month to 3 months (Marsh & Smith, 1995). Results from a second study appeared to suggest a slight decrease in frequency of cognitive symptom endorsement from 3 months to 6 months, but this was not statistically investigated (Hou et al., 2012).
All studies employing healthy control groups found a greater extent of cognitive complaints in mTBI patients relative to controls (Anderson, 2021; Clarke et al., 2012; Mayer et al., 2015; Shumskaya et al., 2012). This was the case early after injury and in the chronic phase post-injury.
In the studies employing injured control groups, three found no differences in cognitive complaint between mTBI and control groups (Clarke et al., 2012; Landre et al., 2006; Norman et al., 2019). These studies were conducted at a range of time points post-injury, at less than 1 week, 3–12 weeks and 3–12 months post-injury. A fourth study found that on day 1 following injury, mTBI patients were 39 times more likely to report concentration complaints than trauma controls, but the odds difference between groups was non-significant by day 8 post-injury (Pacella et al., 2018). The study also found no difference in concentration difficulties between mTBI patients and ‘head injured’ controls who did not meet criteria for mTBI.
With regard to the assessment of individual cognitive domains, most studies reported this data in the form of frequencies of symptom endorsement. The two domains most commonly assessed individually were memory (n = 3; Hou et al., 2012; Raz et al., 2011; Stulemeijer et al., 2007) and concentration (n = 3; Hou et al., 2012; Pacella et al., 2018; Stulemeijer et al., 2007). Only one study reported frequency of endorsement of processing speed symptoms (Hou et al., 2012). None of the studies individually reported executive function symptom data.
With respect to memory symptoms, the frequency of symptom endorsement ranged from 9% to approximately 30% across studies (Hou et al., 2012; Raz et al., 2011; Stulemeijer et al., 2007). It is noteworthy that these studies used different methods of symptom evaluation, making the data non-equivalent. The higher end of the range (15%–30%) represents studies reporting the percentage of their sample endorsing memory complaints, based on ratings on symptom scales (Hou et al., 2012; Raz et al., 2011). The lower end of this range (9% and 10%) was drawn from a study involving daily self-monitoring of memory symptoms and represents the percentage of the time during the 12-day study period that memory symptoms were experienced (Stulemeijer et al., 2007).
With respect to concentration symptoms, frequency of endorsement ranged from 6% to approximately 60% across studies (Hou et al., 2012; Pacella et al., 2018; Stulemeijer et al., 2007). As with memory symptom data, concentration symptom data was derived using varied approaches, limiting between-study comparison. Point estimates for daily self-monitoring of symptoms fell at the lower end of the range (6% and 11%; Stulemeijer et al., 2007), estimates of frequency of the sample experiencing symptoms fell in the middle of the range (15%–25%; Hou et al., 2012) and estimates of the percentage of a sample experiencing concentration difficulties every day over 14 days fell at the higher end of the range (40%–60%; Pacella et al., 2018). In regards to symptoms over time, the latter study showed that concentration complaints decreased over the first 14 days after injury, with about a 28% reduction each day in the odds of reporting these complaints (Pacella et al., 2018).
Processing speed symptoms were reported by between 15% and 25% of individuals in one mTBI sample, with this range again based on extrapolation from a figure (Hou et al., 2012).
In addition to the studies that reported individual cognitive domain data as frequency data, one study reported this as continuous data, that is, mean scores on a symptom scale (Studerus-Germann et al., 2017). Symptom scores were highest for the items ‘difficulty concentrating’ and ‘difficulty remembering’, lower for ‘feeling slowed down’ and zero for the symptom ‘feeling mentally “foggy”’.
Meta-analysis
A meaningful meta-analysis on frequency data was not feasible as a result of the limited number of studies reporting frequency data, methodological differences between studies (e.g. variation in cognitive domains assessed), lack of control groups employed and lack of availability of numerical outcome data (i.e. where data was reported in figures). Therefore, a single meta-analysis was conducted, synthesising studies reporting continuous data. These studies were also highly varied in their methodology. However, they were consistent in reporting overall cognitive symptom scores rather than differing cognitive domains, and most studies had control data available. We therefore included studies that 1) reported continuous outcome data, and 2) employed a control group, to address the research question, Do patients with mTBI report cognitive symptoms to a greater extent than control groups? Based on the small number of included studies, intended subgroup analyses were unable to be conducted.
A total of six studies were included in the final meta-analysis (Anderson, 2021; Clarke et al., 2012; Landre et al., 2006; Mayer et al., 2015; Norman et al., 2019; Shumskaya et al., 2012). Three of the studies employed healthy controls (Anderson, 2021; Mayer et al., 2015; Shumskaya et al., 2012) and two employed injured controls (Landre et al., 2006; Norman et al., 2019). The remaining study employed both healthy and trauma controls, and in this case the trauma group was used as the control group in the analysis, as this was expected to be a closer comparison (Clarke et al., 2012). The resulting meta-analysis included a total of 208 mTBI participants and 214 control participants (135 healthy controls and 79 injured controls).
Each of the six included studies reported cognitive symptom data for a single time point only; these studies ranged from assessing participants approximately 4–5 days after injury (Landre et al., 2006), to assessing participants 3–12 months after injury (Clarke et al., 2012).
Five different symptom scales were employed across the six studies. Available data from the five studies consisted of cognitive subscores on measures of post-concussive symptoms (Landre et al., 2006; Mayer et al., 2015; Norman et al., 2019; Shumskaya et al., 2012) or total scores on a specific cognitive symptom scale (Anderson, 2021; Clarke et al., 2012). In one case where standard deviations were not reported, they were estimated from interquartile ranges using published methods (Wan et al., 2014).
The results of the meta-analysis are presented in Fig. 2. Given the structure of the symptom scales, scores represent the number of symptoms endorsed in combination with the severity of endorsed symptoms.
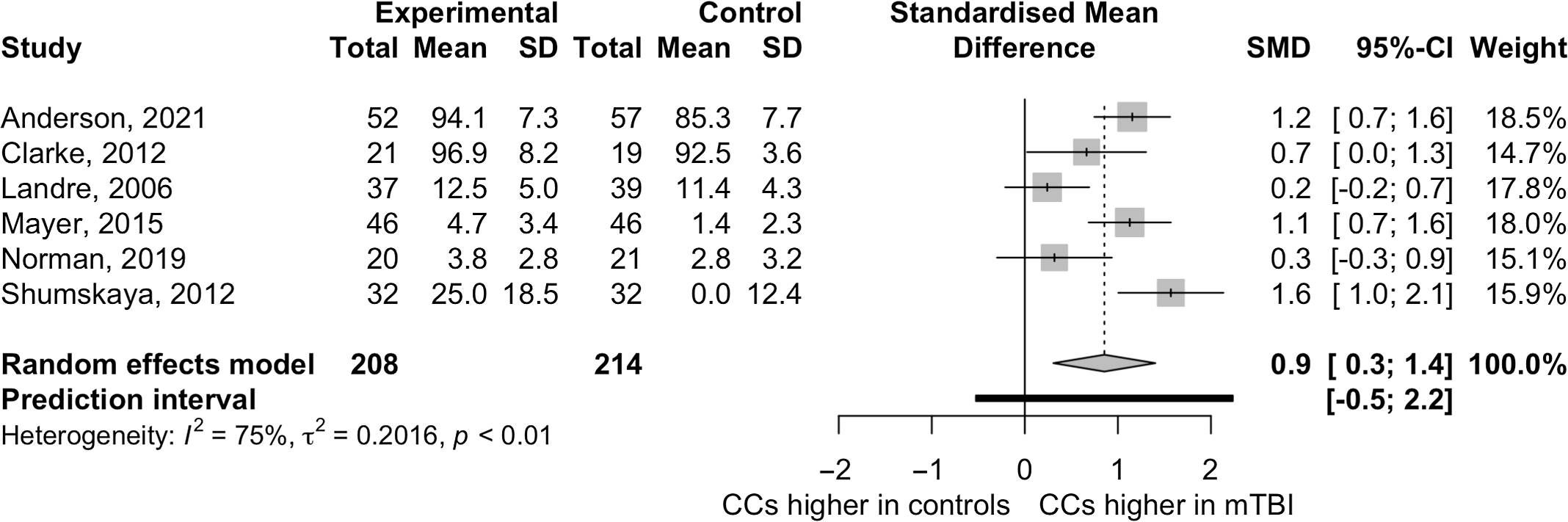
The meta-analysis revealed significant effects for cognitive symptom reporting in mTBI patients versus controls, suggesting that mTBI patients report cognitive symptoms to a greater extent than controls (SMD = 0.85, 95% CI 0.31–1.40, p = .0102). There was a large degree of heterogeneity between studies (τ2 = 0.20, 95% CI 0.04–1.58; I2 = 75.0%, 95% CI 43.4%–89.0%). This was expected due to the methodological differences between studies, including differences in control groups employed and in time post-injury at which assessments took place.
No statistical outliers were detected in the analysis. Statistical tests of publication bias were not conducted given the low power of these tests when the number of included studies is low (Murad, Chu, et al., 2018).
Discussion
This review has demonstrated that cognitive complaints are consistently reported after mTBI, although reported rates differed greatly across studies. Importantly, this study has provided the first meta-analytic evidence to suggest that cognitive complaints are reported to a greater extent (using a combined measure of frequency and severity) in mTBI patients than in control groups. This indicates that cognitive complaints may be specifically elevated in mTBI, in contrast to overall post-concussion symptoms which are typically found to be present at similar levels in mTBI and control groups (Dean et al., 2012; Meares et al., 2011). The current review also highlighted several limitations in the literature, including inconsistencies in methodology between studies and insufficient reporting of study information.
The finding that cognitive complaints occur to a greater extent in mTBI patients than in control groups (in frequency and/or severity) indicates that, after mTBI, cognitive complaints are present beyond ‘normal’ levels. Given cognitive complaints are highly important for successful return to work and extent of healthcare use (Schraa, 1995; Theadom et al., 2017, 2018; Wrightson & Gronwall, 1981), they clearly warrant further attention. Further, whereas measures of overall post-concussion symptoms often do not differ between mTBI and control groups (Dean et al., 2012; Meares et al., 2011), this review suggested that cognitive symptoms, when isolated from other post-concussion symptoms, are specifically elevated in mTBI. Thus, cognitive symptoms may be of specific clinical importance in individuals who are recovering after a mTBI, and deserve further investigation.
The meta-analysis revealed large amounts of heterogeneity between studies, of which underlying causes could not be statistically explored due to insufficient sample size. However, one potentially important source of heterogeneity may have been due to differences in the type of control groups employed. The systematic review revealed that differences in cognitive symptoms between mTBI patients and controls were most often found when healthy controls, rather than injured controls, were employed. This appeared to hold true whether studies were conducted in the acute or chronic phase following injury. Further, in the meta-analysis, the three studies that had the greatest between-group differences were those that employed healthy controls. It is therefore possible that the significant results from the meta-analysis were in part driven by the subgroup of studies that employed healthy controls rather than injured controls.
Due to the limited numbers of studies available for inclusion, the current meta-analysis was unable to determine whether mTBI patients report more cognitive complaints than injured controls specifically. This is an important question to pursue. If there is no difference in cognitive complaints between these groups, it suggests that some of the factors contributing to cognitive complaints in mTBI patients may also be present in injured control patients. In particular, cognitive symptoms may be related to stressors associated with general injury rather than mTBI-related impairment (Cassidy, Cancelliere, et al., 2014). It is also possible, however, that there are factors specific to mTBI which elevate cognitive complaints, either due to true cognitive changes resulting from brain injury or due to psychosocial factors inherent to mTBI (e.g. illness perceptions (Anderson & Fitzgerald, 2018; Whittaker et al., 2007) or ‘diagnosis threat’ (Ozen & Fernandes, 2011)).
With regards to time since injury, findings from the systematic review suggested that cognitive symptoms appear to decrease over time. This aligns with previous research, which has shown that overall post-concussive complaints decrease over time, and that cognitive performance normalises over time (Carroll, Cassidy, Peloso, et al., 2004; Frencham et al., 2005). It is important to consider that the studies included in this review spanned a very wide range with regard to when participants were assessed post-injury, ranging from days to years. Unfortunately, intended subgroup analyses on time since injury could not be conducted due to small sample size. However, given the likely role of time since injury in the reporting of cognitive complaints, it will be important for future studies to investigate this topic in samples that are within discrete post-injury time periods.
With regards to cognitive domains, mTBI patients endorsed symptoms across each of the domains that were individually assessed, that is, memory, attention and processing speed. However, studies varied greatly in regards to how domain-level data was derived, making the data non-equivalent and limiting between-study comparison. Across all included studies, including those that examined domains collectively, memory, attention and processing speed symptoms were commonly assessed. This is consistent with the literature that shows that these are common domains of objective impairment after mTBI (Rabinowitz & Levin, 2014). In contrast, only three of the 13 included studies assessed executive function symptoms, despite this domain also being commonly impaired after mTBI (Frencham et al., 2005; Rabinowitz & Levin, 2014). Given that intended subgroup analyses on type of cognitive complaint were unable to be conducted due to limited sample size, further research is warranted to determine the domain(s) most commonly subjectively impaired after mTBI.
In considering these findings, it is noteworthy that the quality of included studies varied, with four studies meeting less than or equal to 50% of evaluated criteria, and four studies meeting over 80% of evaluated criteria. Similarly, this review found a large degree of inconsistency in methodology between studies, and this was identified as one of the primary methodological issues in the current literature. In particular, inconsistencies and vagueness in defining mTBI have been apparent in the literature for several decades now (Carroll, Cassidy, Holm, et al., 2004; Pertab et al., 2009; Ruff et al., 2009) and this review has shown that these issues remain prevalent.
It is important to note that there were a large number of studies excluded from this review on the basis of the age of included participants. There is a well-established relationship between age and outcome after mTBI, both at the higher and lower ends of the spectrum (Cassidy, Boyle, et al., 2014; Jacobs et al., 2010; Li et al., 2017). Given this relationship, including studies involving older or younger participants – or studies where the age of participants could not be determined – would have created a potential bias for this review. Therefore, to minimise bias, only studies that directly specified that their sample fell between the ages of 18 and 60 were included. Given the impact of age on recovery from mTBI, it is recommended that future studies consider younger and older adults with mTBI as separate, unique populations.
Study limitations
The primary limitation of this systematic review and meta-analysis was small sample size. This resulted in an inability to conduct subgroup analyses, as well as an inability to formally evaluate publication bias. When only a small number of studies are available for quantitative synthesis, limitations primarily include difficulties in accurately estimating meta-analysis parameters (Borenstein et al., 2009). Despite these difficulties, it is still preferable to synthesise studies statistically through meta-analysis in these situations, as this provides for a more accurate representation of data than intuitive ad hoc data summaries, which can be misleading (Borenstein et al., 2009). This limitation was mitigated in the current study through the use of the Hartung–Knapp model adjustment in our meta-analytic approach, which reduces the risk of obtaining a false positive result in the presence of a small number of studies (Inthout et al., 2014). The possibility of small sample sizes within studies was addressed through the use of Hedges’ g, which allows for unbiased estimates of effect size even in the presence of small samples (Borenstein et al., 2009). A final limitation of this study was the absence of a second reviewer for initial screening of relevant literature, due to the large number of studies identified for screening. In order to minimise the potential impact of this limitation, any screening decisions that were unclear were discussed with the second and final authors until consensus was reached; a low threshold was used for initiating this discussion.
Directions for future research
Further research is required to determine whether mTBI patients report greater cognitive complaints than injured control groups, and if so, for what time period post-injury. This will have important implications from a rehabilitation perspective, as it would contribute to understanding the relative specificity of cognitive complaint in mTBI, which could assist with patient management.
Current measures of symptom reporting typically combine symptom frequency and symptom severity into a single score. It will be important for future research to examine cognitive complaints in a manner that allows for the evaluation of complaint frequency and severity as separate entities. The disentanglement of these components will allow for understanding of whether increased levels of cognitive complaint in mTBI are a result of increased complaint frequency, increased complaint severity or both.
Future research would also benefit from executive function difficulties being routinely included in symptom assessment, to enable comprehensive investigation of cognitive symptoms. Similarly, future research would profit from thorough reporting of study information including: age ranges of included participants, how exposure to mTBI was determined, rates of participant follow-up and recruitment setting and selection procedure for control groups. Future studies are encouraged to control for factors known to impact symptom reporting, including sex and psychological factors. Direct adherence to standardised definitions of mTBI, for example, the World Health Organization definition (Carroll, Cassidy, Holm, et al., 2004), would further improve comparability between studies.
Conclusions
This study has confirmed that cognitive complaints are consistently reported after mTBI. Findings have provided clear evidence to suggest that these complaints are reported to a greater extent, using a combined measure of frequency and severity, in mTBI patients than in control groups. Results suggest that this difference in symptom reporting may be greater when healthy controls, rather than injured controls, are employed. Given the importance of elevations in cognitive symptom reporting for outcome after mTBI, including in the context of return to work and healthcare use (Donovan et al., 2014; Theadom et al., 2017), it is evident that cognitive complaints warrant investigation. It is clear from this review, however, that there has been limited research regarding the nature and time course of cognitive complaint after mTBI. Future research into cognitive complaint, including examination of the factors contributing to these complaints, will provide an evidence-based context for clinicians to consider these complaints with respect to management and intervention.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/BrImp.2022.19
Data availability
Data and analysis code is available at the Open Science Framework and can be accessed at: https://osf.io/ckjg6/?view_only=b582da431f6b4bd98ed9998eddd0cb5d.
Acknowledgements
We would like to acknowledge: Jacquie Eyres, who acted as the second reviewer on this project; and Cameron Patrick (Melbourne Statistical Consulting Platform), who provided statistical consulting on this project.
Financial support
This work was supported by a Melbourne Research Scholarship from the University of Melbourne, awarded to the first author.
Conflicts of interest
Arielle M. Levy has no conflicts of interest to disclose. Michael M. Saling has no conflicts of interest to disclose. Jacqueline F. I. Anderson has no conflicts of interest to disclose.
References
Anderson, J. F. I. (2021) Cognitive complaint and objective cognition during the post-acute period after mild traumatic brain injury in pre-morbidly healthy adults. Brain Injury 00(00), 1-11.
| Crossref | Google Scholar |
Anderson, J. F. I., Fitzgerald, P. (2018) Associations between coping style, illness perceptions and self-reported symptoms after mild traumatic brain injury in prospectively studied pre-morbidly healthy individuals. Neuropsychological Rehabilitation 2011, 1-14.
| Crossref | Google Scholar |
Anderson, J. F. I., Jordan, A. S. (2021) Sex predicts post-concussion symptom reporting, independently of fatigue and subjective sleep disturbance, in premorbidly healthy adults after mild traumatic brain injury. Neuropsychological Rehabilitation 0(0), 1-16.
| Crossref | Google Scholar |
Balduzzi, S., Rücker, G., Schwarzer, G. (2019) How to perform a meta-analysis with R: A practical tutorial. Evidence-Based Mental Health 22, 153-160.
| Crossref | Google Scholar |
Beauchamp, F., Boucher, V., Neveu, X., Ouellet, V., Archambault, P., Berthelot, S., Le Sage, N. (2021) Post-concussion symptoms in sports-related mild traumatic brain injury compared to non-sports-related mild traumatic brain injury. Canadian Journal of Emergency Medicine 23(2), 223-231.
| Crossref | Google Scholar |
Cargin, J. W., Collie, A., Masters, C., Maruff, P. (2008) The nature of cognitive complaints in healthy older adults with and without objective memory decline. Journal of Clinical and Experimental Neuropsychology 30(2), 245-257.
| Crossref | Google Scholar |
Carroll, L. J., Cassidy, J. D., Holm, L., Kraus, J., Coronado, V. G. (2004) Methodological issues and research recommendations for mild traumatic brain injury: The WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabilitation Medicine 36(Suppl. 43), 113-125.
| Crossref | Google Scholar |
Carroll, L. J., Cassidy, J. D., Peloso, P. M., Borg, J., Von Holst, H., Holm, L., Pépin, M. (2004) Prognosis for mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabilitation Medicine 36(Suppl. 43), 84-105.
| Crossref | Google Scholar |
Cassidy, J. D., Boyle, E., Carroll, L. J. (2014) Population-based, inception cohort study of the incidence, course, and prognosis of mild traumatic brain injury after motor vehicle collisions. Archives of Physical Medicine and Rehabilitation 95(3, Suppl. 2), S278-S285.
| Crossref | Google Scholar |
Cassidy, J. D., Cancelliere, C., Carroll, L. J., Côté, P., Hincapié, C. A., Holm, L. W., Borg, J. (2014) Systematic review of self-reported prognosis in adults after mild traumatic brain injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Archives of Physical Medicine and Rehabilitation 95(3, Suppl. 2), S132-S151.
| Crossref | Google Scholar |
Cassidy, J. D., Carroll, L. J., Peloso, P. M., Borg, J., Von Holst, H., Holm, L., Coronado, V. G. (2004) Incidence, risk factors and prevention of mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabilitation Medicine 36(Suppl. 43), 28-60.
| Crossref | Google Scholar |
Chapman, J. C., Diaz-Arrastia, R. (2014) Military traumatic brain injury: A review. Alzheimer’s and Dementia 10, S97-S104.
| Crossref | Google Scholar |
Clarke, L. A., Genat, R. C., Anderson, J. (2012) Long-term cognitive complaint and post-concussive symptoms following mild traumatic brain injury: The role of cognitive and affective factors. Brain Injury 26(3), 298-307.
| Crossref | Google Scholar |
Cnossen, M. C., van der Naalt, J., Spikman, J. M., Nieboer, D., Yue, J. K., Winkler, E. A., Lingsma, H. (2018) Prediction of persistent post-concussion symptoms following mild traumatic brain injury. Journal of Neurotrauma 35(22), 2691-2698.
| Crossref | Google Scholar |
Dean, P. J. A., O’Neill, D., Sterr, A. (2012) Post-concussion syndrome: Prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Injury 26(1), 14-26.
| Crossref | Google Scholar |
Deeks, J., Dinnes, J., D’Amico, R., Sowden, A., Sakarovitch, C., Song, F., Altman, D. (2003) Evaluating non-randomised intervention studies. Health Technology Assessment 7(27), iii-109.
| Crossref | Google Scholar |
Donovan, J., Cancelliere, C., Cassidy, J. D. (2014) Summary of the findings of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Chiropractic & Manual Therapies 22(1), 38.
| Crossref | Google Scholar |
Eisenberg, M. A., Meehan, W. P., Mannix, R. (2014) Duration and course of post-concussive symptoms. Pediatrics 133(6), 999-1006.
| Crossref | Google Scholar |
Frencham, K. A. R., Fox, A. M., Maybery, M. T. (2005) Neuropsychological studies of mild traumatic brain injury: A meta-analytic review of research since 1995. Journal of Clinical and Experimental Neuropsychology 27(3), 334-351.
| Crossref | Google Scholar |
Harrer , M. Cuijpers , P. Furukawa , T. Ebert , D. D. 2019 http://dmetar.protectlab.org.
Hartling, L., Hamm, M., Milne, A., Vandermeer, B., Santaguida, P. L., Ansari, M., Dryden, D. M. (2012) Validity and inter-rater reliability testing of quality assessment instruments. Agency for Healthcare Research and Quality www.effectivehealthcare.ahrq.gov/reports/final.cfm.
| Google Scholar |
Higgins, J. P. T., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Retrieved form www.handbook.cochrane.org.
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., Altman, D. G. (2003) Measuring inconsistency in meta-analyses. British Medical Journal 327(7414), 557-560.
| Crossref | Google Scholar |
Hou, R., Moss-Morris, R., Peveler, R., Mogg, K., Bradley, B. P., Belli, A. (2012) When a minor head injury results in enduring symptoms: A prospective investigation of risk factors for postconcussional syndrome after mild traumatic brain injury. Journal of Neurology, Neurosurgery and Psychiatry 83(2), 217-223.
| Crossref | Google Scholar |
Hu, T., Hunt, C., Ouchterlony, D. (2017) Is age associated with the severity of post–mild traumatic brain injury symptoms? Canadian Journal of Neurological Sciences 44(04), 384-390.
| Crossref | Google Scholar |
Inthout, J., Ioannidis, J. P., Borm, G. F. (2014) The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Medical Research Methodology 14(1), 1-12.
| Crossref | Google Scholar |
Iverson, G. L., Karr, J. E., Gardner, A. J., Silverberg, N. D., Terry, D. P. (2019) Results of scoping review do not support mild traumatic brain injury being associated with a high incidence of chronic cognitive impairment: Commentary on McInnes et al. 2017. PLoS ONE 14(9), 1-20.
| Crossref | Google Scholar |
Iverson, G. L., Lange, R. T. (2003) Examination of “postconcussion-like” symptoms in a healthy sample. Applied Neuropsychology 10(3), 137-144.
| Crossref | Google Scholar |
Jacobs, B., Beems, T., Stulemeijer, M., van Vugt, A. B., van der Vliet, T. M., Borm, G. F., Vos, P. E. (2010) Outcome prediction in mild traumatic brain injury: Age and clinical variables are stronger predictors than CT abnormalities. Journal of Neurotrauma 27(4), 655-668.
| Crossref | Google Scholar |
Landre, N., Poppe, C. J., Davis, N., Schmaus, B., Hobbs, S. E. (2006) Cognitive functioning and postconcussive symptoms in trauma patients with and without mild TBI. Archives of Clinical Neuropsychology 21(4), 255-273.
| Crossref | Google Scholar |
Lawley, C. M., Lain, S. J., Algert, C. S., Ford, J. B., Figtree, G. A., Roberts, C. L. (2015) Prosthetic heart valves in pregnancy, outcomes for women and their babies: A systematic review and meta-analysis protocol. BJOG: An International Journal of Obstetrics and Gynaecology 122(11), 1446-1455.
| Crossref | Google Scholar |
Li, W., Risacher, S. L., McAllister, T. W., Saykin, A. J. (2017) Age at injury is associated with the long-term cognitive outcome of traumatic brain injuries. Alzheimer’s and Dementia: Diagnosis, Assessment and Disease Monitoring 6, 196-200.
| Crossref | Google Scholar |
Machamer, J., Temkin, N., Dikmen, S., Nelson, L. D., Barber, J., Hwang, P., Zafonte, R. (2022) Symptom frequency and persistence in the first year after traumatic brain injury: A TRACK-TBI study. Journal of Neurotrauma 39(5–6), 358-370.
| Crossref | Google Scholar |
Marsh, N. V., Smith, M. D. (1995) Post-concussion syndrome and the coping hypothesis. Brain Injury 9(6), 553-562.
| Crossref | Google Scholar |
Mayer, A. R., Hanlon, F. M., Dodd, A. B., Ling, J. M., Klimaj, S. D., Meier, T. B. (2015) A functional magnetic resonance imaging study of cognitive control and neurosensory deficits in mild traumatic brain injury. Human Brain Mapping 36(11), 4394-4406.
| Crossref | Google Scholar |
McCrea, M., Iverson, G. L., McAllister, T. W., Hammeke, T. A., Powell, M. R., Barr, W. B., Kelly, J. P. (2009) An integrated review of recovery after mild traumatic brain injury (MTBI): Implications for clinical management. Clinical Neuropsychologist 23(8), 1368-1390.
| Crossref | Google Scholar |
McHugh, M. L. (2012) Interrater reliability: The kappa statistic. Biochemia Medica 22(3), 276-282.
| Crossref | Google Scholar |
Meares, S., Shores, E. A., Batchelor, J., Baguley, I. J., Chapman, J., Gurka, J., Marosszeky, J. E. (2006) The relationship of psychological and cognitive factors and opioids in the development of the postconcussion syndrome in general trauma patients with mild traumatic brain injury. Journal of the International Neuropsychological Society 12(6), 792-801.
| Crossref | Google Scholar |
Meares, S., Shores, E. A., Taylor, A. J., Batchelor, J., Bryant, R. A., Baguley, I. J., Marosszeky, J. E. (2011) The prospective course of postconcussion syndrome: The role of mild traumatic brain injury. Neuropsychology 25(4), 454-465.
| Crossref | Google Scholar |
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., Altman, D., Antes, G., Tugwell, P. (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine 6(7),.
| Crossref | Google Scholar |
Murad, M. H., Chu, H., Lin, L., Wang, Z. (2018) The effect of publication bias magnitude and direction on the certainty in evidence. BMJ Evidence-Based Medicine 23(3), 84-86.
| Crossref | Google Scholar |
Murad, M. H., Sultan, S., Haffar, S., Bazerbachi, F. (2018) Methodological quality and synthesis of case series and case reports. Evidence-Based Medicine 23(2), 60-63.
| Crossref | Google Scholar |
Ngwenya, L. B., Gardner, R. C., Yue, J. K., Burke, J. F., Ferguson, A. R., Huang, M. C., Manley, G. T. (2018) Concordance of common data elements for assessment of subjective cognitive complaints after mild-traumatic brain injury: A TRACK-TBI Pilot Study. Brain Injury 32(9), 1071-1078.
| Crossref | Google Scholar |
Norman, R. S., Shah, M. N., Turkstra, L. S. (2019) Reaction time and cognitive-linguistic performance in adults with mild traumatic brain injury. Brain Injury 33(9), 1173-1183.
| Crossref | Google Scholar |
Ozen, L. J., Fernandes, M. A. (2011) Effects of “diagnosis threat” on cognitive and affective functioning long after mild head injury. Journal of the International Neuropsychological Society 17(2), 219-229.
| Crossref | Google Scholar |
Pacella, M., Prabhu, A., Morley, J., Huang, S., Suffoletto, B. (2018) Postconcussive symptoms over the first 14 days after mild traumatic brain injury: An experience sampling study. Journal of Head Trauma Rehabilitation 33(3), E31-E39.
| Crossref | Google Scholar |
Pertab, J. L., James, K. M., Bigler, E. D. (2009) Limitations of mild traumatic brain injury meta-analyses. Brain Injury 23(6), 498-508.
| Crossref | Google Scholar |
Pullens, M. J. J., De Vries, J., Roukema, J. A. (2010) Subjective cognitive dysfunction in breast cancer patients: A systematic review. Psycho-Oncology 19(11), 1127-1138.
| Crossref | Google Scholar |
R Core Team (2019). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. Retrieved from https://www.R-project.org/.
Rabinowitz, A. R., Levin, H. S. (2014) Cognitive sequelae of traumatic brain injury. Psychiatric Clinics of North America 37(1), 1-11.
| Crossref | Google Scholar |
Raz, E., Jensen, J. H., Ge, Y., Babb, J. S., Miles, L., Reaume, J., Inglese, M. (2011) Brain iron quantification in mild traumatic brain injury: A magnetic field correlation study. American Journal of Neuroradiology 32, 1851-1856.
| Google Scholar |
Ruff, R. M., Iverson, G. L., Barth, J. T., Bush, S. S., Broshek, D. K. (2009) Recommendations for diagnosing a mild traumatic brain injury: A National Academy of Neuropsychology education paper. Archives of Clinical Neuropsychology 24(1), 3-10.
| Crossref | Google Scholar |
Schneider, A. L. C., Huie, J. R., Boscardin, W. J., Nelson, L., Barber, J. K., Yaffe, K., Gardner, R. C. (2022) Cognitive outcome 1 year after mild traumatic brain injury. Neurology 98(12), e1248-e1261.
| Crossref | Google Scholar |
Schraa, J. C. (1995) Mild traumatic brain injury: Searching for the syndrome. Journal of Head Trauma Rehabilitation 10(4), 28-40.
| Crossref | Google Scholar |
Shumskaya, E., Andriessen, T. M. J. C., Norris, D. G., Vos, P. E. (2012) Abnormal whole-brain functional networks in homogeneous acute mild traumatic brain injury. Neurology 79(2), 175-182.
| Crossref | Google Scholar |
Stillman, A. M., Madigan, N., Torres, K., Swan, N., Alexander, M. P. (2019) Subjective cognitive complaints in concussion. Journal of Neurotrauma 311, 305-311.
| Crossref | Google Scholar |
Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., Thacker, S. B. (2000) Meta-analysis of observational studies in epidemiology: A proposal for reporting. JAMA 283(15), 2008-2012.
| Crossref | Google Scholar |
Studerus-Germann, A. M., Engel, D. C., Stienen, M. N., von Ow, D., Hildebrandt, G., Gautschi, O. P. (2017) Three versus seven days to return-to-work after mild traumatic brain injury: A randomized parallel-group trial with neuropsychological assessment. International Journal of Neuroscience 127(10), 900-908.
| Crossref | Google Scholar |
Stulemeijer, M., Vos, P. E., Bleijenberg, G., van der Werf, S. P. (2007) Cognitive complaints after mild traumatic brain injury: Things are not always what they seem. Journal of Psychosomatic Research 63(6), 637-645.
| Crossref | Google Scholar |
Sullivan, K. A., Edmed, S. L., Greenslade, J. H., White, M., Chu, K., Lukin, B., Lurie, J. K. (2017) Psychological predictors of postconcussive symptoms following traumatic injury. Journal of Head Trauma Rehabilitation 33(4), 1.
| Crossref | Google Scholar |
Te Ao, B., Brown, P., Tobias, M., Ameratunga, S., Barker-Collo, S., Theadom, A., Feigin, V. L. (2014) Cost of traumatic brain injury in New Zealand: Evidence from a population-based study. Neurology 83(18), 1645-1652.
| Crossref | Google Scholar |
Theadom, A., Barker-Collo, S., Jones, K., Kahan, M., Te Ao, B., McPherson, K., Te Ao, B. (2017) Work limitations 4 years after mild traumatic brain injury: A cohort study. Archives of Physical Medicine and Rehabilitation 98(8), 1560-1566.
| Crossref | Google Scholar |
Theadom, A., Starkey, N., Barker-Collo, S., Jones, K., Ameratunga, S., Feigin, V. (2018) Population-based cohort study of the impacts of mild traumatic brain injury in adults four years post-injury. PLoS ONE 13(1), 1-13.
| Crossref | Google Scholar |
Veritas Health Innovation. (2019). Covidence systematic review software. Melbourne, Australia. Retrieved from www.covidence.org.
Veroniki, A. A., Jackson, D., Viechtbauer, W., Bender, R., Bowden, J., Knapp, G., Kuss, O., Salanti, G. (2016) Methods to estimate the between-study variance and its uncertainty in meta-analysis. Research Synthesis Methods 7(1), 55-79.
| Crossref | Google Scholar |
Voormolen, D. C., Polinder, S., von Steinbuechel, N., Vos, P. E., Cnossen, M. C., Haagsma, J. A. (2019) The association between post-concussion symptoms and health-related quality of life in patients with mild traumatic brain injury. Injury 50(5), 1068-1074.
| Crossref | Google Scholar |
Vos, P. E., Battistin, L., Birbamer, G., Gerstenbrand, F., Potapov, A., Prevec, T., Von Wild, K. (2002) EFNS guideline on mild traumatic brain injury: Report of an EFNS task force. European Journal of Neurology 9(3), 207-219.
| Crossref | Google Scholar |
Wan, X., Wang, W., Liu, J., Tong, T. (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Medical Research Methodology 14(1), 1-13.
| Crossref | Google Scholar |
Wells, G. A., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., & Tugwell, P. (2000). The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Retrieved from https://www.ohri.ca//programs/clinical_epidemiology/oxford.Asp.
Whittaker, R., Kemp, S., House, A. (2007) Illness perceptions and outcome in mild head injury: A longitudinal study. Journal of Neurology, Neurosurgery and Psychiatry 78(6), 644-646.
| Crossref | Google Scholar |
Wickham, H., Averick, M., Bryan, J., Chang, W., McGowan, L., François, R., Yutani, H. (2019) Welcome to the Tidyverse. Journal of Open Source Software 4(43),.
| Crossref | Google Scholar |
Wrightson, P., Gronwall, D. (1981) Time off work and symptoms after minor head injury. Injury 12(6), 445-454.
| Crossref | Google Scholar |
Yousefzadeh-Chabok, S., Kapourchali, F. R., Ramezani, S. (2021) Determinants of long-term health-related quality of life in adult patients with mild traumatic brain injury. European Journal of Trauma and Emergency Surgery 47(3), 839-846.
| Crossref | Google Scholar |
Zeng, X., Zhang, Y., Kwong, J. S. W., Zhang, C., Li, S., Sun, F., Du, L. (2015) The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. Journal of Evidence-Based Medicine 8(1), 2-10.
| Crossref | Google Scholar |
Footnotes
1 Note: The protocol for this systematic review and meta-analysis was preregistered through PROSPERO (registration number: CRD42020151284). Data and analysis code has been made available on the Open Science Framework and can be accessed at: https://osf.io/ckjg6/?view_only=b582da431f6b4bd98ed9998eddd0cb5d.