

Chlamydia retesting remains low among young women in Australia: an observational study using sentinel surveillance data, 2018–2022
Stephanie C. Munari A B * , Anna L. Wilkinson A B C , Jason Asselin A , Louise Owen D , Phillip Read E , Robert Finlayson F , Sarah Martin G H , Charlotte Bell I J , Catherine C. O’Connor K , Allison Carter K L M , Rebecca Guy K , Anna McNulty N , Rick Varma N , Eric P. F. Chow B O P , Christopher K. Fairley O P , Basil Donovan K , Mark Stoove A , Jane L. Goller B , Jane Hocking B , Margaret E. Hellard A B Q and
A B * , Anna L. Wilkinson A B C , Jason Asselin A , Louise Owen D , Phillip Read E , Robert Finlayson F , Sarah Martin G H , Charlotte Bell I J , Catherine C. O’Connor K , Allison Carter K L M , Rebecca Guy K , Anna McNulty N , Rick Varma N , Eric P. F. Chow B O P , Christopher K. Fairley O P , Basil Donovan K , Mark Stoove A , Jane L. Goller B , Jane Hocking B , Margaret E. Hellard A B Q and A
B
C
D
E
F
G
H
I
J
K
L
M
N
O
P
Q
Abstract
Chlamydia remains the most notified bacterial sexually transmissible infection in Australia with guidelines recommending testing for re-infection at 3 months post treatment. This paper aimed to determine chlamydia retesting and repeat positivity rates within 2–4 months among young women in Australia, and to evaluate what factors increase or decrease the likelihood of retesting.
Chlamydia retesting rates among 16–29-year-old women were analysed from Australian Collaboration for Coordinated Enhanced Sentinel Surveillance of sexually transmissible infection and bloodborne virus (ACCESS) sentinel surveillance data (n = 62 sites). Among women with at least one positive test between 1 January 2018 and 31 August 2022, retesting counts and proportions within 2–4 months were calculated. Logistic regression was performed to assess factors associated with retesting within 2–4 months.
Among 8758 women who were positive before 31 August 2022 to allow time for follow up, 1423 (16.2%) were retested within 2–4 months, of whom 179 (12.6%) tested positive. The odds of retesting within 2–4 months were 25% lower if tested in a coronavirus disease 2019 (COVID-9) pandemic year (2020–2022) (aOR = 0.75; 95% CI 0.59–0.95). Among 9140 women with a positive test before 30 November 2022, 397 (4.3%) were retested too early (within 7 days to 1 month) and 81 (20.4%) of those were positive.
Chlamydia retesting rates remain low with around a sixth of women retested within 2–4 months in line with guidelines. Re-infection is common with around one in eight retesting positive. An increase in retesting is required to reduce the risk of reproductive complications and onward transmission.
Keywords: chlamydia, primary care, re-infection, retesting, sexual health, sexually transmissible infection, surveillance, women.
Introduction
In Australia, chlamydia is the most frequently notified sexually transmissible infection (STI) with 86 916 notifications occurring in 2021.1 Around two-thirds of notifications (n = 60 563) occurred among people aged 15–29 years, and half (n = 44 547) among women.1 As over 85% of chlamydia infections are asymptomatic,2 many people are unaware of their infection, which may persist for over a year.3 Chlamydia infections in people with female reproductive organs (from here on, the term women will be used) can lead to complications in the form of pelvic inflammatory disease (PID), chronic pelvic pain, ectopic pregnancy and infertility.4 Repeat infections are common with data from Australian primary care estimating a cumulative risk of re-infection of 20.3% among women aged 15–25 years within 5 months following treatment.5 Furthermore, each repeat infection increases the risk of PID by 20%.6 Past analyses of Australian sentinel surveillance data have shown low retesting and high re-infection rates following chlamydia infection. In mainstream primary care clinics (general practice) during 2008–2009, 24.6% of 16–29–year–olds were retested within 1.5–4 months (19% tested positive)7 and in specialist sexual health clinics during 2004–2008, 17.8% of heterosexual women were retested within 1–4 months (16.1% tested positive).8 Another study found 20.6% of women aged 15–29 years with chlamydia in 2016 were retested within 1.4–6 months.9
Increasingly, there has been a shift towards an enhanced case management approach to chlamydia that focuses on retesting and partner management, in light of evidence that widespread opportunistic screening is unlikely to reduce chlamydia prevalence.10,11 An important component of this approach involves retesting women at 3 months following a positive test to detect re-infection, as recommended in Australian STI testing guidelines.12 Repeat testing at 3 months allows for earlier treatment if a repeat infection is detected and an opportunity to reduce the likelihood of reproductive complications.13
In this retrospective cohort study, we sought to provide updated patterns in chlamydia retesting and repeat positivity for young women in Australia, with a particular focus on timely retesting (defined as within 2–4 months) as recommended by Australian STI guidelines.12 Findings are intended to evaluate current chlamydia retesting patterns in Australia and to strengthen the case for action to increase retesting rates within 2–4 months as part of a multi–pronged approach to reduce the burden of chlamydia in Australia.
Materials and methods
Setting
Data were obtained from the Australian Collaboration for Coordinated Enhanced Sentinel Surveillance of STIs and bloodborne viruses (BBVs) (ACCESS, accessproject.org.au). ACCESS is a sentinel surveillance system comprised of 114 sites including general practices, community and sexual health clinics, hospitals, laboratories and drug and alcohol services from each state and territory in Australia who see a high proportion of people at greater risk of STIs (chlamydia, gonorrhoea, syphilis) and BBVs (human immunodeficiency virus, hepatitis B virus and hepatitis C virus). ACCESS aims to monitor the testing, diagnosis and treatment of STIs and BBVs and to evaluate strategies aimed at reducing their transmission.14
Data collection and management
Deidentified routine clinical and testing data were retrospectively extracted from patient management systems at participating ACCESS sites using GRHANITE data extraction software. Data included in this study were obtained for the calendar years 2018–2022 from ACCESS site types including sexual health clinics, general practices who provide care to the general community, general practices who specialise in the care of gay and bisexual men (GBM) and community health clinics. Data items included age group, sexuality (including whether a women was ever flagged as bisexual, homosexual or heterosexual within the ACCESS dataset), sex and gender (including whether a women was ever flagged as transgender or other sex within the ACCESS dataset), ACCESS site type, having ever identified as a sex worker, patient location (metropolitan or non-metropolitan, where non-metropolitan included regional, rural and remote areas) based on their most recent postcode of residence using the Australian Statistical Geography Standard remoteness area classification, and patient country of birth, categorised as Australia or overseas. Data collected within ACCESS are what is routinely available within the electronic medical record system of participating clinics, thus completeness of some data items varied between types of clinical settings.
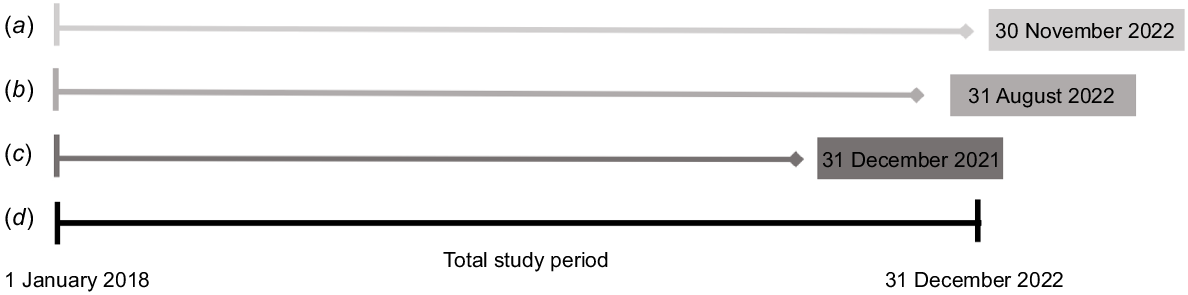
Data were included for women aged between 16 and 29 years who had at least one positive chlamydia test from any anatomical site (genitourinary, rectal or oral) during the period from 1 January 2018 to 30 November 2022, with a woman’s first positive test in the study period representing the starting point of follow up for that woman. A second test in the data set was defined as the next chlamydia test taken from any anatomical site that occurred immediately subsequent to a baseline positive test and before 31 December 2022, with no other chlamydia tests performed in between. The primary outcome was to determine retesting that occurred on time in accordance with Australian testing guidelines, which recommend retesting at 3 months12 and to evaluate what factors increase or decrease the probability of retesting on time. In order to provide leeway for retesting to occur, a range of 2–4 months of a first positive chlamydia test was selected for our primary outcome and women with a first positive test up until 31 August 2022 were followed up. We also calculated repeat positivity for women retested on time. Sub-analyses investigated the following secondary outcomes: (1) retesting that occurred too early (from 7 days to 1 month of a positive chlamydia test) as tests performed this early are at increased risk of a false-positive result from persistent chlamydia DNA (even if performed as a test of cure in pregnant people and those with an anorectal infection treated with azithromycin12), for which women with a first positive test up until 30 November 2022 were followed up until 31 December 2022; and (2) to determine the distribution of retest occurrence in the 12 months following a positive chlamydia test, for which women with a first positive test until 31 December 2021 were followed up until 31 December 2022. Within ACCESS, tests that occur within 7 days are collapsed into one test event, so a positive test represents a 7-day window. A schematic of timelines for the analyses is shown in Fig. 1.
Timeline of cut-off dates by which a woman’s first positive test needed to occur for sub-analyses. (a) Women who had a second test performed within 1 month, (b) women who had a second test performed within 2–4 months, (c) women who had a second test performed within 12 months, and (d) total study period.
Analysis
The number of clinics and tests performed at each ACCESS site type was calculated for all women with at least one positive chlamydia test within the study period between 1 January 2018 and 31 December 2022. Retesting patterns were analysed by year, coronavirus disease 2019 (COVID-19) year (defined as 2020–2022), age group, sexuality, sex and gender, ACCESS site type, having ever identified as a sex worker, patient location and country of birth. All analyses were performed using R statistical software (ver. 4.2.1) and Microsoft Excel (ver. 16.77).
Counts and proportions were calculated for the number of women retested and re-infected within 1 month and within 2–4 months of their first positive test. To explore factors associated with women receiving guidelines-based testing (retesting at 3 months to detect re-infection), regression modelling was used to evaluate the odds of retesting within 2–4 months, adjusting for the above demographic factors. The demographic variables of sex worker status, patient location and patient country of birth were excluded from the multivariate logistic regression post hoc to reduce confounding given the large number of incomplete data.
For women who had a retest within 12 months of their first positive test, the ACCESS site type where their first positive test occurred was compared to the site where their second positive test occurred, and the number of concordant pairs (tests that occurred at the same site type) and discordant pairs (tests that occurred at different site types) were counted. Descriptive statistics, including a histogram, were performed to visualise the distribution of retest occurrences over 12-months using the time in months between first and second positive test.
Ethics approval
Ethics approval for ACCESS was provided by the Human Research Ethics Committees at Alfred Hospital (248/17), Central Australia (CA−19–3355), Northern Territory Department of Health and Menzies School of Health (08/47), University of Tasmania (H0016971), Aboriginal Health and Medical Research Council (1099/15), ACON (2015/14), Victorian AIDS Council/Thorne Harbour Health (VAC REP 15/003) and St. Vincent’s Hospital (08/051).
Results
Overall, 9253 women aged 16–29 years had at least one positive chlamydia test within the study period from 1 January 2018 to 31 December 2022. Among the 9253 women within the total study period, 162 (1.8%) and 16 (0.2%) were ever flagged as transgender or other sex, respectively. Among the same 9253 women, 899 (9.7%) were ever flagged as bisexual only; 65 (0.7%) as homosexual only; 6500 (70.2%) as heterosexual only; with the remainder a combination of the three sexuality variables and no missing data. The number of ACCESS clinics and chlamydia tests contributed by ACCESS site type for the entire study period is in Table 1.
| Number of clinics | Number of women who had ≥1 positive chlamydia test | ||
|---|---|---|---|
| n | n (%) | ||
| Sexual health clinics | 23 | 7645 (82.6%) | |
| General practices who provide care to the general community | 16 | 526 (5.7%) | |
| General practices who specialise in the care of gay and bisexual men | 16 | 254 (2.7%) | |
| Community health clinics | 7 | 828 (8.9%) | |
| Total | 62 | 9253 |
Among 8758 women who had their first positive test before 31 August 2022 and contributed to the analysis of our primary outcome of retesting within 2–4 months, most were aged 20–24 years (n = 4453, 50.8%), resided in metropolitan areas (n = 6050, 69.1%) and attended a sexual health clinic for testing (n = 7226, 82.5%). A total of 849 participants (9.7%) identified as having ever worked as a sex worker. Table 2 provides a breakdown of the proportions retested and retesting positive within 2–4 months and within 1 month by year and demographic characteristics. For our secondary outcomes of retesting within 1 month and within 12 months of their first positive test, population demographics for these women were very similar to those who had a retest within 2–4 months (Table 2). A schematic of timelines for the analyses is shown in Fig. 1 and a flowchart describing the number of women retested by study outcome in shown in Fig. S1.
| Second test within 2–4 months | Second test within 1 month | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥1 positive test before 31 August 2022 | Second test within 2–4 months | Proportion with second test within 2–4 months (95% CI) | Second test within 2–4 months and positive | Proportion positive when second test within 2–4 months (95% CI) | ≥1 positive test before 30 November 2022 | Second test within 1 month | Proportion with second test within 1 month (95% CI) | Second test within 1 month and positive | Proportion positive when second test within 1 month (95% CI) | ||
| n | n | % | n | % | n | n | % | n | % | ||
| Total | 8758 | 1423 | 16.2 (15.5–17.0) | 179 | 12.6 (10.9–14.3) | 9140 | 397 | 4.3 (3.9–4.8) | 81 | 20.4 (16.4–24.4) | |
| Year | |||||||||||
| 2018 | 2652 | 463 | 17.5 (16.0–18.9) | 62 | 13.4 (10.3–16.5) | 2652 | 129 | 4.9 (4.0–5.7) | 30 | 23.3 (16.0–30.5) | |
| 2019 | 2584 | 433 | 16.8 (15.3–18.2) | 52 | 12.0 (8.9–15.1) | 2584 | 96 | 3.7 (3.0–4.4) | 18 | 18.8 (10.9–26.6) | |
| 2020 | 1520 | 203 | 13.4 (11.6–15.1) | 21 | 10.3 (6.2–14.5) | 1520 | 77 | 5.1 (4.0–6.2) | 14 | 18.2 (9.6–26.8) | |
| 2021 | 1170 | 187 | 16.0 (13.9–18.1) | 25 | 13.4 (8.5–18.2) | 1170 | 47 | 4.0 (2.9–5.1) | 9 | 19.1 (7.9–30.4) | |
| 2022 | 832 | 137 | 16.5 (13.9–19.0) | 19 | 13.9 (8.1–19.7) | 1214 | 48 | 4.0 (2.9–5.1) | 10 | 20.8 (9.3–32.3) | |
| COVID-19 test year | |||||||||||
| No | 5236 | 896 | 17.1 (16.1–18.1) | 114 | 12.7 (10.5–14.9) | 5236 | 225 | 4.3 (3.7–4.8) | 48 | 21.3 (16.0–26.7) | |
| Yes | 3522 | 527 | 15.0 (13.8–16.1) | 65 | 12.3 (9.5–15.1) | 3904 | 172 | 4.4 (3.8–5.0) | 33 | 19.2 (13.3–25.1) | |
| Age group (years) | |||||||||||
| 16–19 | 1204 | 201 | 16.7 (14.6–18.8) | 30 | 14.9 (10.0–19.9) | 1253 | 50 | 4.0 (2.9–5.1) | 13 | 26.0 (13.8–38.2) | |
| 20–24 | 4453 | 735 | 16.5 (15.4−17.6) | 104 | 14.0 (11.6–16.7) | 4668 | 189 | 4.0 (3.5–4.6) | 42 | 22.2 (16.3–28.1) | |
| 25–29 | 3101 | 487 | 15.7 (14.4−17.0) | 45 | 9.2 (6.7–11.8) | 3219 | 158 | 4.9 (4.2–5.7) | 26 | 16.5 (10.7–22.2) | |
| ACCESS site type | |||||||||||
| SHC | 7226 | 1164 | 16.1 (15.3−17.0) | 142 | 12.2 (10.3–14.1) | 7545 | 277 | 3.7 (3.2–4.1) | 57 | 20.6 (15.8–25.3) | |
| CH | 793 | 147 | 18.5 (15.8–21.2) | 24 | 16.3 (10.4–22.3) | 822 | 46 | 5.6 (4.0−7.2) | 14 | 30.4 (17.1–43.7) | |
| GP GBM | 240 | 46 | 19.2 (14.2–24.1) | 5 | 10.9 (1.9–19.9) | 252 | 22 | 8.7 (5.2–12.2) | 5 | 22.7 (5.2–40.2) | |
| GP | 499 | 66 | 13.2 (10.3–16.2) | 8 | 12.1 (4.2–20.0) | 521 | 52 | 10.0 (7.4–12.6) | 5 | 9.6 (1.6–17.6) | |
| Ever sex worker | |||||||||||
| Yes | 849 | 199 | 23.4 (20.6–26.3) | 19 | 9.5 (5.5–13.6) | 869 | 59 | 6.8 (5.1–8.5) | 14 | 23.7 (12.9–34.6) | |
| No | 3431 | 565 | 16.5 (15.2–17.7) | 83 | 14.7 (11.8–17.6) | 3589 | 126 | 3.5 (2.9–4.1) | 30 | 23.8 (16.4–31.2) | |
| Missing | 4478 | 659 | 14.7 (13.7–15.8) | 77 | 11.7 (9.2–14.1) | 4682 | 212 | 4.5 (3.9–5.1) | 37 | 17.5 (12.3–22.6) | |
| Patient location | |||||||||||
| Metro | 6050 | 977 | 16.1 (15.2−17.1) | 118 | 12.1 (10.0–14.1) | 6303 | 302 | 4.8 (4.3–5.3) | 61 | 20.2 (15.7–24.7) | |
| Non-metro | 1480 | 280 | 18.9 (16.9–20.9) | 37 | 13.2 (9.2–17.2) | 1544 | 48 | 3.1 (2.2–4.0) | 12 | 25.0 (12.8–37.2) | |
| Missing | 1228 | 166 | 13.5 (11.6–15.4) | 24 | 14.5 (9.1–19.8) | 1293 | 47 | 3.6 (2.6–4.7) | 8 | 17.0 (6.3–27.8) | |
| Patient country of birth | |||||||||||
| Australia | 3479 | 584 | 16.8 (15.5–18.0) | 71 | 12.2 (9.5–14.8) | 3670 | 128 | 3.5 (2.9–4.1) | 28 | 21.9 (14.7–29.0) | |
| Overseas | 3581 | 559 | 15.6 (14.4–16.8) | 68 | 12.2 (9.5–14.9) | 3702 | 145 | 3.9 (3.3–4.5) | 28 | 19.3 (12.9–25.7) | |
| Missing | 1698 | 280 | 16.5 (14.7–18.3) | 40 | 14.3 (10.2–18.4) | 1768 | 124 | 7.0 (5.8–8.2) | 25 | 13.1 (13.1–27.2) | |
CI, confidence interval; SHC, sexual health clinic; CH, community health; GP GBM, general practice specialising in the care of gay and bisexual men; GP, general practice.
Retesting within 2–4 months
Of the 8758 women who had their first positive test before 31 August 2022, 16.2% (n = 1423, 95% CI 15.5–17.0%) received a retest within 2–4 months of whom 12.6% (n = 179, 95% CI 10.9–14.3%) had a positive retest (Table 2).
Results for the frequency of retesting within 2–4 months and the univariable and multivariable analysis are provided in Tables 2 and 3. The proportion retested within 2–4 months was higher in the years prior to the COVID-19 pandemic (2018 and 2019) at 17.1% (95% CI 16.1–18.1%) compared to during the COVID-19 pandemic (2020, 2021 and 2022) at 15.0% (95% CI 13.8–16.1%). The proportion retested was similar between age-groups (16–19 years 16.7% (95% CI 14.6–18.8%), 20–24 years 16.5% (95% CI 15.4–17.6%), 25–29 years 15.7% (95% CI 14.4–17.0)) and was higher for women who had ever identified as a sex-worker (23.4%, 95% CI 20.6–26.3) than for women who had never identified as a sex worker (16.5%, 95% CI 15.2–17.7%). The retesting proportion was also higher for women living in non-metropolitan (18.9%, 95% CI 16.9–20.9%) than in metropolitan areas (16.1%, 95% CI 15.2–17.1%) and for Australian born women (16.8%, 95% CI 15.5–18.0%) than for overseas born women (15.6%, 95% CI 14.4–16.8%). Multivariable logistic regression estimated that women had a 25% reduction in odds of being retested within 2–4 months if tested in a COVID-19 pandemic year (adjusted odds ratio (aOR) = 0.75; 95% CI 0.59–0.95). The multivariable analysis was adjusted for year, COVID-19 test year, age group and ACCESS site type (Table 3).
| Variable | ≥1 positive test before 31 August 2022 | Second test within 2–4 months | Proportion with second test within 2–4 months | Univariable | Multivariable A | |||
|---|---|---|---|---|---|---|---|---|
| n | n | % | OR | 95% CI | aOR | 95% CI | ||
| Year | 8758 | 1423 | 16.2 | 0.96 | 0.92–1.01 | 1.06 | 0.97–1.16 | |
| COVID-19 test year | ||||||||
| No | 5236 | 896 | 17.1 | Ref | Ref | |||
| Yes | 3522 | 527 | 15.0 | 0.85 | 0.76–0.96 | 0.75 | 0.59–0.95 | |
| Age group (years) | ||||||||
| 16–19 | 1204 | 201 | 16.7 | Ref | Ref | |||
| 20–24 | 4453 | 735 | 16.5 | 0.99 | 0.83–1.17 | 1.00 | 0.84–1.19 | |
| 25–29 | 3101 | 487 | 15.7 | 0.93 | 0.78–1.11 | 0.95 | 0.79–1.14 | |
| ACCESS site type | ||||||||
| SHC | 7226 | 1164 | 16.1 | Ref | – | Ref | – | |
| CH | 793 | 147 | 18.5 | 1.19 | 0.98–1.43 | 1.18 | 0.97–1.43 | |
| GBM GP | 240 | 46 | 19.2 | 1.23 | 0.89–1.71 | 1.25 | 0.90–1.74 | |
| GP | 499 | 66 | 13.2 | 0.79 | 0.61–1.04 | 0.81 | 0.62–1.06 | |
| Ever sex worker | ||||||||
| No | 849 | 199 | 23.4 | Ref | – | Ref | ||
| Yes | 3431 | 565 | 16.5 | 1.55 | 1.29–1.86 | – | – | |
| Unknown | 4478 | 659 | 14.7 | 0.88 | 0.77–0.99 | – | – | |
| Patient location | ||||||||
| Metro | 6050 | 977 | 16.1 | Ref | – | Ref | – | |
| Non-metro | 1480 | 280 | 18.9 | 1.21 | 1.05–1.40 | – | – | |
| Missing | 1228 | 166 | 13.5 | 0.81 | 0.68–0.97 | – | – | |
| Patient country of birth | ||||||||
| Australia | 3479 | 584 | 16.8 | Ref | – | Ref | – | |
| Overseas | 3581 | 559 | 15.6 | 0.92 | 0.81–1.04 | – | – | |
| Missing | 1698 | 280 | 16.5 | 0.98 | 0.84–1.14 | – | – | |
OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval; SHC, sexual health clinic; CH, community health; GP GBM, general practice specialising in the care of gay and bisexual men; GP, general practice.
Retests within 1 month
Among the 9140 women who had their first positive chlamydia test before 30 November 2022, 4.3% (95% CI 3.9–4.8%) received a second test within 7 days and within 1 month. Among those retested within 1 month, 20.4% (95% CI 16.4–24.4%) had a positive retest (Table 2).
Distribution of second tests within 12 months
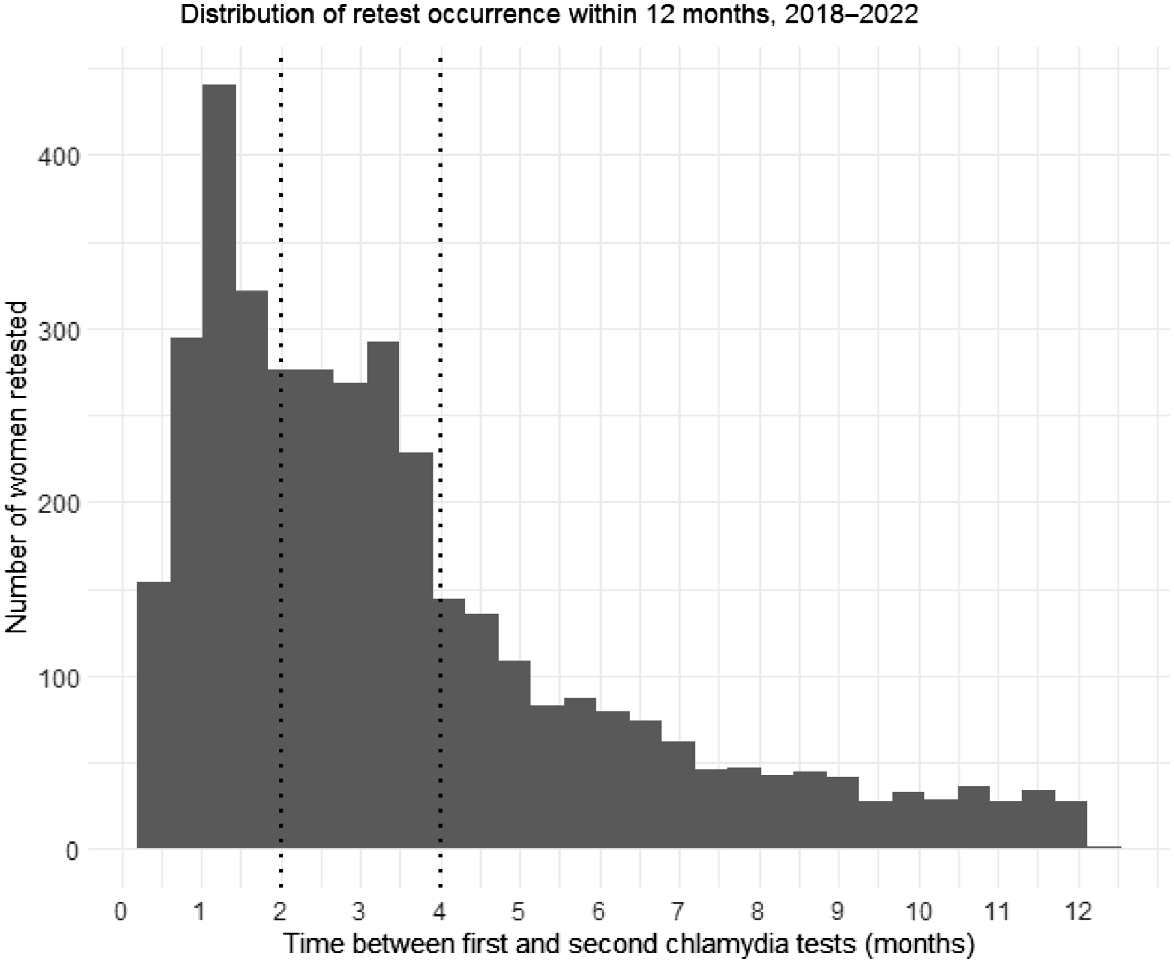
Overall, among those who had their first positive chlamydia test between 1 January 2018 and 31 December 2021, the median time to retest was 86.0 days (IQR 46.0–140.8 days) with 69% of retests occurring within 4 months (Fig. 2).
Histogram showing the distribution of retest occurrence within 12 months of a woman’s first positive chlamydia test that occurred between 1 January 2018 and 31 December 2021. Dotted vertical lines indicate 2 months and 4 months.
Among the 4228 women who had their first positive test before 31 December 2021 and their second test within the remaining study period, only 96 (2.3%) had their second test at a discordant ACCESS site type e.g. first test at a sexual health clinic and second test at a general practice.
Discussion
Among women attending STI and BBV sentinel surveillance sites in Australia with at least one positive chlamydia test between January 2018 to August 2022, we observed that only 16.2% had a repeat test within 2–4 months, as recommended in Australian STI testing guidelines. Among women retested within 2–4 months, 12.6% tested positive. Retesting on time was lower during COVID-19 pandemic years (2020–2022) compared to non-COVID-19 years. Few women were retested too early but 20.4% of those retested within a month tested positive. In the 12 months after a positive chlamydia test, most repeat tests occurred within the first 4 months. These findings reinforce current testing guidelines that recommend that patients with a positive chlamydia test be retested at 3 months to identify a persistent or new infection (re-infection), to initiate repeat treatment and reduce the likelihood of reproductive complications.
Our finding of 16.2% of women retested and 12.6% with a repeat positive test within 2–4 months is slightly lower than previously reported in Australia,7–9 even prior to the onset of the COVID-19 pandemic. The lower retesting rates observed in this study may be due to the ACCESS system now having a larger number and different composition of clinical sites compared to when it commenced. For example, the early ACCESS system included family planning clinics, that may be more likely to retest patients. Additionally, concerted efforts to increase chlamydia testing as part of an overall chlamydia response, including a multifaceted chlamydia testing intervention were underway in Australia between 2010 and 2015.11 It is also possible that some patients who tested positive during a COVID-19 pandemic year, were advised to delay their retest due to community lockdowns and may contribute to lower retesting during this period. In our univariable analysis, we also found that retesting within 2–4 months was more likely for women who identified as a sex worker or resided in non-metropolitan areas. Higher retesting rates among women who had ever identified as a sex worker is likely influenced by mandatory STI testing regulations in various state and territories.15 Of note, there is no evidence that sex workers in Australia have higher STI rates compared to the general population, with the Australian sex industry adopting safer sex practices through advocacy, peer-based education and support and outreach services.16 Although guidelines recommend regular STI and BBV testing, sex workers may request more frequent testing to comply with workplace and other local legal frameworks.16 The repeal of mandatory requirements to undergo regular 3-monthly STI testing in Victoria as of May 2022 is likely to alter this outcome in future years.17 The higher odds of retesting for women residing in non-metropolitan areas may reflect a combination of higher GP chlamydia testing rates in non-metropolitan areas18 and people residing in regional or rural areas being more likely to attend the same clinic or a clinic in the same area.19 Importantly, a higher proportion of positive retests occurred within 1 month of an initial positive test compared to those retested within 2–4 months. This may represent false-positive tests due to persistent chlamydia DNA and are likely being performed too early. Additionally, given that most chlamydia tests in this analysis were performed at sexual health clinics, it is possible that women are being referred back to their primary care physician for retesting, and thus contributing to low overall retesting rates. This may be acting as an additional barrier and represent a missed opportunity for retesting to occur. Further exploration into the feasibility of sexual health clinics playing a greater role in chlamydia retesting is required.
In addition to providing an update to chlamydia retesting figures in Australia, the strengths of this study include the assessment of multiple site types from around Australia including sexual health clinics, general practices and community health clinics, along with offering insights into individual-level factors associated with retesting in accordance with Australian guidelines; a comparison of retesting both before and during the COVID-19 pandemic; and a particular focus on women, who are disproportionately burdened by the reproductive complications associated with chlamydia infections. However, there are important considerations to note when interpreting our findings. First, being a sentinel surveillance system, sites represented in this analysis see a larger proportion of people at greater risk of STIs, reflected by sexual health clinics contributing more than 80% of our testing data. Second, women may have been retested at another site not participating in ACCESS or, for travellers, returned to their home country before retesting could occur, and therefore not had their retest observed in our data. This would result in an underestimation of the true rate of retesting. Third, as test events that occur within 7 days are collapsed into one event within ACCESS, if a woman had a second test within 7 days of their first positive test and did not have another chlamydia test for the remaining study period, their second test would not have been captured. This would result in an overestimation of the number of women who did not receive a second test in the study period, when in fact they did receive a second test it just occurred too early. Fourth, caution should be exercised when attributing a person’s second positive test as a true re-infection. Given that guidelines do not recommend a test of cure, except for pregnant people and anorectal infection treated with azithromycin,12 it is difficult to differentiate re-infection from a persistent primary infection. Fifth, as there was a large number of incomplete data for some demographic variables such as sex worker status, patient location and country of birth, these factors were not included in multivariable logistic regression analyses. Finally, generalisability of the findings should be limited to countries and regions with similar access to primary care and testing services as Australia.
As part of a suite of interventions to reduce the morbidity from chlamydia, increasing retesting within 2–4 months following a positive test can have significant individual and population level benefits by reducing the risk of reproductive complications and onward transmission. An Australian modelling study has estimated a reduction in the prevalence of chlamydia from 4.6% to 2.6% over 4 years when, in addition to increasing testing coverage, the proportion retested within 4 months of treatment is doubled from the rate achieved in a large cluster–randomised controlled trial among heterosexual 16–29-year-olds in Australia.20 Additional modelling estimated that 22% of all-cause PID could be prevented by annual chlamydia testing intervals.21 Combined with the knowledge that each repeat chlamydia infection increases the risk of PID by 20%,6 the importance of prompt retesting in a population already at a higher risk of re-infection cannot be understated. Interventions aiming to increase chlamydia retesting, including patient text message reminders and postal home collection kits, have been shown to increase retesting rates within 1–4 months of a chlamydia diagnosis.22,23 Studies such as the Management of Chlamydia Cases in Australia trial24 are underway to ascertain how best to implement such strategies within the complex and competing priorities of the primary care environment, where many STIs are diagnosed and managed.19 In addition to increasing retesting, a greater understanding of what women perceive as the risks and consequences of re-infection is required, as part of a multipronged approach to reducing the health impacts from chlamydia acquisition.
Our findings have demonstrated that chlamydia retesting within 2–4 months among young women, as recommended in Australian STI testing guidelines, continues to be low, with repeat infections common. These findings reinforce the importance of adhering to current testing guidelines to promptly detect re-infection and commence treatment. In the context of an increasing paradigm shift towards an enhanced case management approach to reduce reproductive complications from chlamydia,25,26 improved retesting is one way in which we can work towards reducing the burden of chlamydia in Australia.
Participant consent
As our study analyses de–identified data collected under the auspices of public health surveillance, individual patient consent was not required. Individuals were able to opt–out of the surveillance system if they wished.
Data availability
The data that support this study cannot be publicly shared due to ethical or privacy reasons and may be shared upon reasonable request to the corresponding author if appropriate.
Conflicts of interest
Margaret Hellard receives funding from Gilead Science and Abbvie for investigator–initiated research unrelated to this area of work. Eric Chow is an Associate Editor of Sexual Health. To mitigate this potential conflict of interest they were blinded from the review process. All other authors declare no conflicts of interest.
Declaration of funding
Stephanie Munari is supported by a Burnet Institute PhD scholarship, Jane Hocking is supported by a National Health and Medical Research Council (NHMRC) Senior Research Fellowship (GNT1042907), Margaret Hellard is supported by an NHMRC Investigator Grant (GNT1194322) and Eric P. F. Chow is supported by an NHMRC Emerging Investigator Grant (GNT1172873). ACCESS receives core funding from the Australian Department of Health with the aim to monitor Australia’s progress in the control of bloodborne viruses and sexually transmitted infections. In addition, the governments of New South Wales, Victoria, and Western Australia provide funding for state level outcomes. Funding for particular outcomes is also provided by the Blood Borne Virus & STI Research, Intervention and Strategic Evaluation Program (BRISE), an NHMRC Project Grant (APP1082336), a NHMRC Partnership Grant (GNT1092852), and the Prevention Research Support Program, funded by the New South Wales Ministry of Health. No funding body played a role in the planning, writing or publication of this manuscript.
Acknowledgements
The authors acknowledge the contribution of the ACCESS Team members who are not co–authors of this article including: Htein Linn Aung, Kirby Institute, UNSW Sydney; Wayne Dimech, NRL; Alexis Apostolellis, Australasian Society for HIV Medicine; Aaron Cogle, National Association of People with HIV Australia; Brendan Quinn, Victoria Department of Health; Clare Bradley, ATLAS; Daniel Coase, Federation of Ethnic Communities’ Councils of Australia (FECCA); Dash Heath-Paynter, Health Equity Matters (AFAO); David Lewis, Western Sydney Sexual Health Centre; David Nolan, Royal Perth Hospital; David Templeton, Royal Prince Alfred Hospital; Edward Huddy, Ministry of Health; Emma Sanguineti, Queensland Ministry of Health; Florin Douglas, Deakin University; Janaki Amin, NSW Ministry of Health; Jane Davies, Menzies School of Health Research; John Didlick, Hepatitis Australia; John G, Australian Injecting and Illicit Drug Users League (AIVL); Jess Doumany, Australian Injecting and Illicit Drug Users League; Lisa Bastian, WA Department of Health; Mandy Charleton, Ministry of Health; Manoji Gunathilake, Royal Darwin Hospital; Megan Campbell, National Aboriginal Community Controlled Health Organisation (NAACHO); Mish Pony, Scarlet Alliance; Norm Roth, Prahran Market Clinic; Philip Cunningham, SydPath; Tom Rees, SA Ministry of Health; Greta Baillie, Kirby Institute, UNSW Sydney; Thi Nguyen, Burnet Institute; Victoria Polkinghorne, Burnet Institute; Michael Traeger, Burnet Institute; Nyssa Watson, Burnet Institute. The authors also acknowledge all clinics participating in ACCESS, including the site investigators who contributed data to this analysis. ACCESS is a partnership between the Burnet Institute, Kirby Institute and NRL Quality.
References
2 Peipert JF. Clinical practice. Genital chlamydial infections. N Engl J Med 2003; 349(25): 2424-2430.
| Crossref | Google Scholar | PubMed |
3 Geisler WM. Duration of untreated, uncomplicated Chlamydia trachomatis genital infection and factors associated with chlamydia resolution: a review of human studies. J Infect Dis 2010; 201(S2): 104-113.
| Crossref | Google Scholar |
4 Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. J Infect Dis 2010; 201(S2): 134-155.
| Crossref | Google Scholar |
5 Walker J, Tabrizi SN, Fairley CK, Chen MY, Bradshaw CS, Twin J, et al. Chlamydia trachomatis incidence and re-infection among young women – behavioural and microbiological characteristics. PLoS ONE 2012; 7(5): e37778.
| Crossref | Google Scholar | PubMed |
6 Davies B, Ward H, Leung S, Turner KME, Garnett GP, Blanchard JF, et al. Heterogeneity in risk of pelvic inflammatory diseases after chlamydia infection: a population-based study in Manitoba, Canada. J Infect Dis 2014; 210(suppl 2): S549-S555.
| Crossref | Google Scholar | PubMed |
7 Bowring AL, Gouillou M, Guy R, Kong FYS, Hocking J, Pirotta M, et al. Missed opportunities—low levels of chlamydia retesting at Australian general practices, 2008–2009. Sex Transm Infect 2012; 88(5): 330-334.
| Crossref | Google Scholar | PubMed |
8 Guy R, Wand H, Franklin N, Fairley CK, Chen MY, O’Connor CC, et al. Re-testing for chlamydia at sexual health services in Australia, 2004-08. Sex Health 2011; 8(2): 242-7.
| Crossref | Google Scholar | PubMed |
9 Gray RT, Callander D, Hocking JS, McGregor S, McManus H, Dyda A, et al. Population-level diagnosis and care cascade for chlamydia in Australia. Sex Transm Infect 2020; 96(2): 131-136.
| Crossref | Google Scholar | PubMed |
10 van Bergen JEAM, Hoenderboom BM, David S, Deug F, Heijne JCM, van Aar F, et al. Where to go to in chlamydia control? From infection control towards infectious disease control. Sex Transm Infect 2021; 97(7): 501-506.
| Crossref | Google Scholar | PubMed |
11 Hocking JS, Temple-Smith M, Guy R, Donovan B, Braat S, Law M, et al. Population effectiveness of opportunistic chlamydia testing in primary care in Australia: a cluster-randomised controlled trial. Lancet 2018; 392(10156): 1413-1422.
| Crossref | Google Scholar | PubMed |
12 Australian STI Management Guidelines For Use In Primary Care. Chlamydia. 2022. Available at https://sti.guidelines.org.au/sexually-transmissible-infections/chlamydia/ [cited 5 January 2023]
13 Herzog SA, Althaus CL, Heijne JCM, Oakeshott P, Kerry S, Hay P, et al. Timing of progression from Chlamydia trachomatis infection to pelvic inflammatory disease: a mathematical modelling study. BMC Infect Dis 2012; 12: 187.
| Crossref | Google Scholar | PubMed |
14 Callander D, Moreira C, El-Hayek C, Asselin J, van Gemert C, Watchirs Smith L, et al. Monitoring the control of sexually transmissible infections and blood-borne viruses: protocol for the Australian Collaboration for Coordinated Enhanced Sentinel Surveillance (ACCESS). JMIR Res Protoc 2018; 7(11): e11028.
| Crossref | Google Scholar | PubMed |
15 Australasian Society for HIV Viral Hepatitis and Sexual Health Medicine (ASHM). Sex work. 2019. Available at https://hivlegal.ashm.org.au/sex-work/ [cited 14 July 2023]
16 Australian STI Management Guidelines For Use In Primary Care. Sex workers. 2021. Available at https://sti.guidelines.org.au/populations-and-situations/sex-workers/ [ cited 19 September 2023]
17 Victorian Government. Decriminalising sex work in Victoria. Victorian Government; 2023. Available at https://www.vic.gov.au/sex-work-decriminalisation [cited 28 June 2023]
18 Kong FYS, Guy RJ, Hocking JS, Merritt T, Pirotta M, Heal C, et al. Australian general practitioner chlamydia testing rates among young people. Med J Aust 2011; 194(5): 249-252.
| Crossref | Google Scholar | PubMed |
19 Yeung AH, Temple-Smith M, Fairley CK, Vaisey AM, Guy R, Law MG, et al. Chlamydia prevalence in young attenders of rural and regional primary care services in Australia: a cross-sectional survey. Med J Aust 2014; 200(3): 170-175.
| Crossref | Google Scholar | PubMed |
20 Hui BB, Hocking JS, Braat S, Donovan B, Fairley CK, Guy R, et al. Intensified partner notification and repeat testing can improve the effectiveness of screening in reducing Chlamydia trachomatis prevalence: a mathematical modelling study. Sex Transm Infec 2022; 98(6): 414-419.
| Crossref | Google Scholar | PubMed |
21 Price MJ, Ades AE, Soldan K, Welton NJ, Macleod J, Simms I, et al. The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis. Health Technol Assess 2016; 20(22): 1-250.
| Crossref | Google Scholar | PubMed |
22 Smith KS, Hocking JS, Chen MY, Fairley CK, McNulty AM, Read P, et al. Dual intervention to increase chlamydia retesting: a randomized controlled trial in three populations. Am J Prev Med 2015; 49(1): 1-11.
| Crossref | Google Scholar | PubMed |
23 Downing SG, Cashman C, McNamee H, Penney D, Russell DB, Hellard ME. Increasing chlamydia test of re-infection rates using SMS reminders and incentives. Sex Transm Infect 2013; 89(1): 16-19.
| Crossref | Google Scholar | PubMed |
24 Goller JL, Coombe J, Temple-Smith M, Bittleston H, Sanci L, Guy R, et al. Management of Chlamydia Cases in Australia (MoCCA): protocol for a non-randomised implementation and feasibility trial. BMJ Open 2022; 12(12): e067488.
| Crossref | Google Scholar | PubMed |
25 Unemo M, Bradshaw CS, Hocking JS, de Vries HJC, Francis SC, Mabey D, et al. Sexually transmitted infections: challenges ahead. Lancet Infect Dis 2017; 17(8): e235-e279.
| Crossref | Google Scholar | PubMed |
26 Coombe J, Goller J, Vaisey A, Bourne C, Sanci L, Bateson D, et al. New best practice guidance for general practice to reduce chlamydia-associated reproductive complications in women. Aust J Gen Pract 2021; 50(1–2): 50-54.
| Crossref | Google Scholar | PubMed |