

‘Every strategy needs to be contributing to erasing the stigma’: Māori and Pacific young people talk about overcoming barriers to testing for sexually transmitted infections
Sally B. Rose A * , Abby Dunlop A , Tracey Gardiner A , Marama Cole A , Susan M. Garrett A and Eileen M. McKinlay A
A * , Abby Dunlop A , Tracey Gardiner A , Marama Cole A , Susan M. Garrett A and Eileen M. McKinlay A
A
Abstract
Māori and Pacific young people are disproportionately impacted by sexually transmitted infections (STIs). Access to STI screening is important to reduce transmission and reproductive health complications.
Between November 2022 and May 2023, we held four wānanga (workshops) with Māori and Pacific participants (15–24 years old) to find out what barriers they encounter to STI testing, and hear their ideas about how to overcome these. Participants were recruited via youth-focused community organisations in the Wellington region of Aotearoa New Zealand. Inductive thematic analysis was used to understand data generated from discussions, drawing on Māori and Pacific models of wellbeing to frame themes.
Thirty-eight participants were involved in the wānanga. Barriers to STI testing related to five themes: (1) differences in cultural values and expression; (2) family/friends; (3) educational gaps; (4) psychological factors; and (5) structural obstacles. Suggested strategies to improve access to sexual health care included the need for free, flexible services, education and health promotion activities to reach young people in their spaces (e.g. church, marae, social media). Participants stressed the need for approaches to be community-based, delivered by trusted individuals using culturally appropriate messages, and saw participation in STI testing as beneficial for whānau/family and communities.
To improve access to STI testing, participants described the need for free services, together with education and health promotion to improve inter-generational sexual health knowledge. Reframing messages around STIs to align with Māori and Pacific models of wellbeing was identified as a way to normalise conversations, in turn reducing the stigma surrounding STI testing.
Keywords: chlamydia, gonorrhoea, health promotion, Māori, Pacific, sexual health, sexually transmitted infections (STIs), young people.
Introduction
All young people have a right to sexual and reproductive health and wellbeing.1 To empower and support their right to self-determination over their sexual health, young people need access to quality information, relationship and sexuality education as well as free and confidential sexual and reproductive health services.1,2 Sexual health guidelines recommend at least annual chlamydia and gonorrhoea screening for all sexually active under 30-year-olds.3 Chlamydia and gonorrhoea infections are often asymptomatic, so screening is important to detect and treat infection to reduce short- and long-term adverse outcomes. Sexual health and reproductive health are closely linked; chlamydia, gonorrhoea and syphilis all have implications for future fertility, and can adversely affect pregnancy outcomes. Long-term complications of untreated chlamydia or gonorrhoea include pelvic inflammatory disease, ectopic pregnancy and infertility; infection can be passed to the baby in pregnancy or at birth, and there is increased risk of acquiring and passing on HIV and human papillomavirus.4,5 Syphilis in pregnancy is associated with a high risk of adverse pregnancy outcomes including miscarriage, stillbirth, neonatal death and congenital syphilis in a live-born infant.6 All these infections can be effectively treated with antibiotics once detected.3
In Aotearoa New Zealand (NZ), population case rates of bacterial sexually transmitted infections (STIs, for example chlamydia and gonorrhoea) are consistently highest among young people aged 15–29 years, and for Māori (the indigenous people of NZ) and Pacific (communities with origins or ancestors from Polynesia, Melanesia and Micronesia) young people; rates are two to three times higher than those experienced by European/other ethnicities.7 Despite this, Māori and Pacific youth are tested at proportionately lower rates than European/other ethnicities.8 This higher burden of undetected, untreated infection places Māori and Pacific young people at greater risk for reproductive health complications including the possibility of ectopic pregnancy and infertility.9 The number of syphilis cases among reproductive aged women (15–44 years) has been rising in Aotearoa, and a disproportionate number of cases diagnosed since 2020 have been Māori women, and almost all cases of congenital syphilis in 2022 were Māori infants.10 These unacceptable inequities stem from socio-economic and social determinants of health as well as structural barriers such as limited access to quality, culturally appropriate sexual health information and services, gaps in individual health provider competencies, and an overall lack of investment in culturally appropriate education and health promotion.11,12
International research has identified a range of reasons that young people are unable to access STI testing that are broadly related to patient, provider and system-level factors.13–16 Relatively few studies have explored barriers to STI testing in Aotearoa, but research involving University students in Wellington and an online survey of young people in Hawke’s Bay showed that negative societal attitudes and stigma surrounding sex and sexuality, confidentiality concerns, fear of judgement, shame, cost and not knowing where to go all hindered access to sexual health care.17–19 Qualitative research involving rangatahi Māori (young people) in the Waikato region has identified multiple social and structural barriers that limit access to information and services to support good sexual health.2,20 Cost and transport barriers are common for those living rurally,20 and takatāpui (Māori term to describe diverse sexualities, gender and sex characteristics) rangatahi report fear of discrimination by health professionals related to their sexual orientation or gender identity.2 For Pacific young people, cultural values and religion influences how sex, sexuality and reproduction are viewed, which likely further limits their ability to engage with sexual health care.21
Māori and Pacific young people are among those considered priority groups that require specific, tailored approaches to reduce and eliminate STI-related inequities.22 Recognising them as the experts in their own lives and their right to good sexual and reproductive health, we sought Māori and Pacific young peoples’ ideas on overcoming barriers to STI testing.
Materials and methods
Participants and recruitment
To support participant recruitment, we undertook stakeholder engagement to seek practical advice and contacts of people or groups that might be willing to assist with recruitment in the Wellington region. Over 6 months, we met with 10 Māori and Pacific adults working in the community as educators, health promoters, youth workers, and school nurses. This resulted in successful links with four (non-health related) organisations that provide services, support, wellbeing and resilience programs to Māori and Pacific rangatahi. These organisations approached potential participants, explained the study and obtained signed informed consent on our behalf. Eligibility criteria are: age 16–24 years; Māori and/or Pacific ethnicities; and willing to share views about sexual health in a group setting.
The University of Otago Human Ethics Committee (Health) approved this study on 31 January 2022 (REF H22/003).
Wānanga overview and data generation
We ran four wānanga (workshops) for four different groups of rangatahi between November 2022 and May 2023. Wānanga were facilitated by three members of our research team: (1) TG, Pākehā; (2) AD, Sāmoan/Palagi (European); and (3) MC, Māori/Pākehā. All were cis-female aged in their 30s and 40s with a mix of experience related to youth health, mental health, midwifery, Pacific and Māori health and co-design research.
Three meetings were held at the community organisation venues and one in a local marae (Māori meeting house). In Groups 1, 2, and 4, a team member of the organisation was present for parts of the wānanga, while in Group 3, the organisation team member stayed nearby but not in the same room. Wānanga ran for 1.5–3.5 h, dependant on group availability. Participants in Groups 3 and 4 were not in education, employment or training (NEET) and involved in readiness to work/train/study programs. They took part in our wānanga immediately after one of their scheduled meetings so these wānanga were shorter in duration. Participants received a $NZD200 gift card in recognition of their contribution to the research.
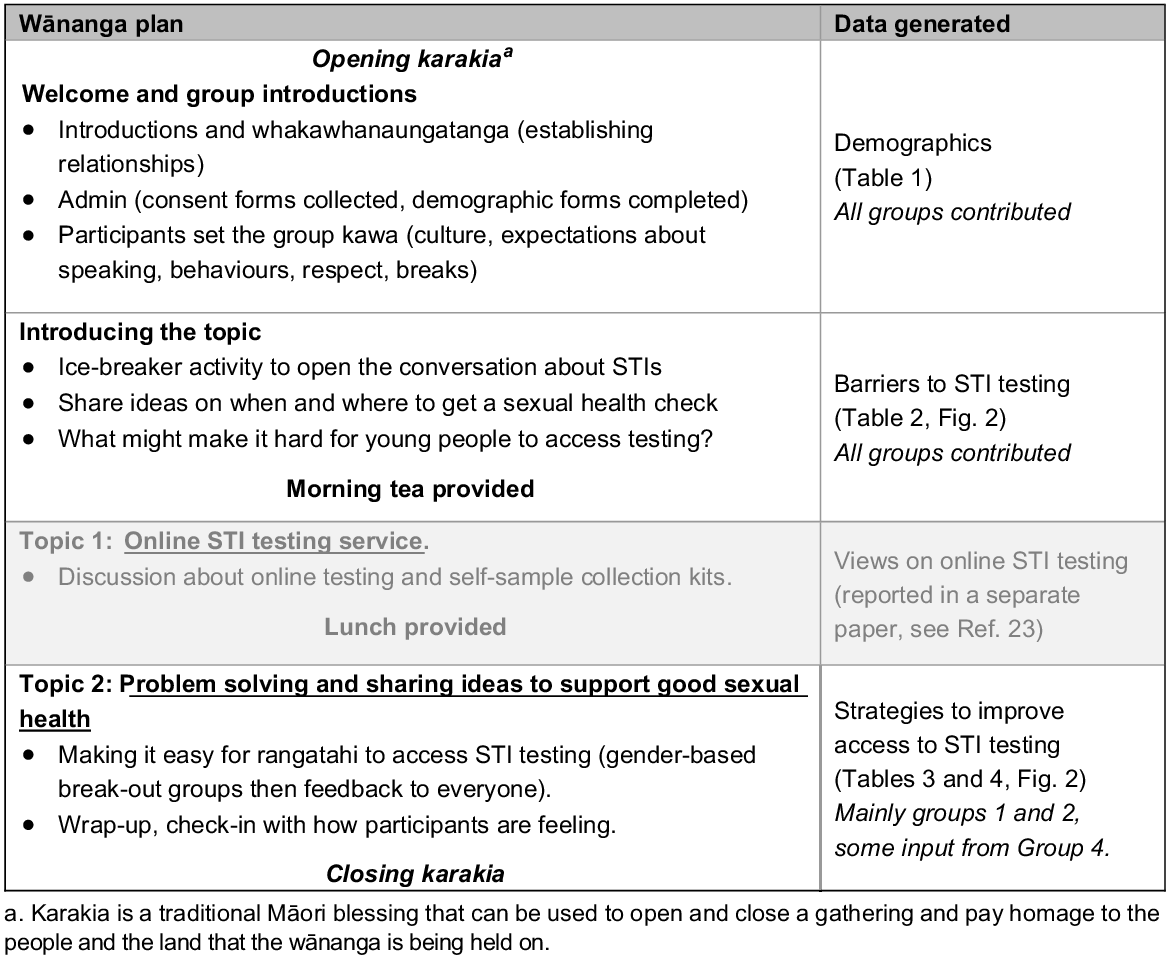
Fig. 1 shows an overview of the plan used to guide wānanga. Discussion was split into two parts: (1) views towards online STI testing (reported separately);23 and (2) understanding and overcoming barriers in access to STI testing (presented here). Participants were asked to imagine they worked in the community and had been tasked with coming up with practical ways to overcome some of the barriers they had identified as limiting access to STI testing. Wānanga concluded by inviting participants to share something they had learnt or that stood out, how they felt at the end of the session and plans for the rest of the day. A local, evidence-based website about sexual health was shared, and pamphlets on STI testing offered in English and Māori. Facilitators had contact details for support organisations in case any participant expressed a need for information or support (no-one did).
Wānanga were audio-recorded, and ideas generated in group discussion were captured by participants as written group work notes. The first two meetings were transcribed verbatim by two members of the research team, the third and fourth (shorter meetings) were transcribed using Sonix AI software with a member of the team manually correcting any content errors in pertinent parts of the transcript by re-listening to the audio. Team member AD took fieldnotes throughout each wānanga and undertook rapid analysis immediately afterwards to generate bullet-point summaries.
Data analysis
We used an inductive thematic analytical approach, starting with data familiarisation (reading transcripts and summaries) followed by an iterative coding process, development and refinement of themes.24 Lead facilitator TG undertook initial coding, with subsequent review and additions by AD and SR. A table was produced with broad topic headings and subheadings incorporating codes, short notes and selected quotes from transcripts. This was then split into two tables: one related to barriers to STI testing; and the other with content related to overcoming barriers. Theoretical coding was then undertaken by AD (Sāmoan) for data related to barriers to STI testing. Data were grouped thematically drawing on two holistic models of health and wellbeing: (1) the Pacific Fonofale model;25 and (2) the Te Whare Tapa Whā Māori model.26 The Fonofale model provides a way of conceptualising Pacific wellbeing using the fale (traditional Sāmoan house) to represent the different constructs of health.25 Developed by Karl Pulotu-Endemann in 1984, this model recognises the importance of interconnected Pacific values (family, culture and beliefs, spiritual, physical, mental and other aspects of wellbeing) together with surrounding influences such as time, environmental and context.25 Similarly, the Te Whare Tapa Whā is a model developed by Mason Durie in 1994 that depicts a wharenui (traditional Māori meeting house) to symbolise the strong foundation upon which the four equal walls or dimensions considered important for Māori health and wellbeing sit. These dimensions are: (1) physical; (2) mental and emotional; (3) social (whānau/family, friendships); and (4) spiritual values and beliefs are inter-related and each supports the others.26 Both models recognise that all dimensions are considered as equally important components of a whole, so in the context of sexual health, consideration should be given to the individual and to family, communities, friends and the surrounding environment or context. When discussing strategies to overcome barriers, participants referenced both the Fonofale and Te Whare Tapa Whā models as being important frameworks for the development of health promotion strategies.
Our main findings are presented in tables, with inclusion of a figure that provides a visual overview of results. Quotes were selected to illustrate key themes and ideas and include both unique and more common, shared views. Quotes have been annotated with group number (G1-4), gender (M, F) and speaker ID (number) where possible; however, gender and speaker ID could not be distinguished for all participants. Some quotes were edited for brevity (e.g. removal of fillers, repetition). Several participants are over-represented in the quotes because they were the nominated spokesperson when reporting back following small group discussions.
Results
Participant characteristics
Table 1 describes the demographic characteristics of the 38 participants (15–24 years old) in the four groups. Groups included a mix of ages, genders (60% female), ethnicities (50% Māori, 50% Pacific of whom 14/19 were Sāmoan) and participants who were NEET.
| Self-identified characteristics | Group 1 (n = 10) Duration 3.5 h | Group 2 (n = 8) Duration 3.5 h | Group 3 (n = 14) Duration 2.5 h | Group 4 (n = 6) Duration 1.5 h | Total (n = 38) Duration 11 h | ||
|---|---|---|---|---|---|---|---|
| n | n | n | n | n | % | ||
| Age-band (mean) A | (20.4) | (19.9) | (17.5) | (19.0) | (19.2) | – | |
| 15–16 years | 0 | 0 | 3 | 0 | 3 | 7.9 | |
| 17–18 years | 0 | 2 | 4 | 4 | 10 | 26.3 | |
| 19–20 years | 1 | 3 | 4 | 1 | 9 | 23.7 | |
| 21–22 years | 3 | 3 | 0 | 0 | 6 | 15.8 | |
| 23–24 years | 5 | 0 | 0 | 1 | 6 | 15.8 | |
| Not known B | 1 | 0 | 3 | 0 | 4 | 10.5 | |
| Gender | |||||||
| Female C | 5 | 7 | 6 | 5 | 23 | 60.5 | |
| Male | 5 | 1 | 8 | 1 | 15 | 39.5 | |
| Ethnicity (total count) D | |||||||
| Māori | 3 | 3 | 9 | 4 | 19 | 50.0 | |
| Pacific | 7 | 6 | 2 | 4 | 19 | 50.0 | |
| Not known B | 0 | 0 | 3 | 0 | 3 | 7.9 | |
| Sexual orientation | |||||||
| Straight, heterosexual | 8 | 6 | 10 | 4 | 28 | 73.7 | |
| Gay, bisexual, pansexual | 1 | 1 | 1 | 2 | 5 | 13.2 | |
| Prefer not to say | 1 | 0 | 0 | 0 | 1 | 2.6 | |
| Not known B | 0 | 1 | 3 | 0 | 4 | 10.5 | |
| Ever had a sexual health check | |||||||
| Yes | 5 | 6 | 3 | 2 | 16 | 42.1 | |
| No | 4 | 1 | 7 | 3 | 15 | 39.5 | |
| Don’t know | 1 | 1 | 1 | 1 | 4 | 10.5 | |
| Not known B | 0 | 0 | 3 | 0 | 3 | 7.9 | |
Awareness of STI testing
Overall, 42% of participants reported having had an STI check in the past with variability between groups (ranging from 21% in G3 to 75% in G2). When asked to call out the name of an STI as part an ice-breaker activity to open the conversation about STIs, chlamydia and gonorrhoea were mentioned in all groups and syphilis was mentioned in only one group. There was a general understanding of when to get an STI check, with suggestions including: when sexually active, with a new partner, having multiple partners, suspicions of cheating, or to prevent transmission. However, gaps existed, such as not considering testing during pregnancy, when symptomatic, or when a partner tests positive. There was less certainty about where to get tested. General practitioners or doctors were cited in three groups, while Family Planning and a Youth Health Service were noted in two groups, some asked if self-testing or testing at a pharmacy or hospital were possible and someone said they would Google it. In Group 3, most participants lacked knowledge about where to go, and sexual health clinics or student health services were not brought up in any group.
When invited to share what stood out to them at the end of the session, we saw evidence of increased understanding about STI testing.23 Some participants noted the positive experience of engaging in conversations and sharing opinions about STI testing in their groups. They highlighted an absence of awkwardness during discussions and noted the benefits of hearing others’ perspectives. Several comments suggested that participation in this work had helped dispel fears or misconceptions related to STI testing. For example, people noted that they had learnt how STIs are passed on and that it does not hurt to get an STI check.
Barriers to STI testing and suggested strategies to overcome these
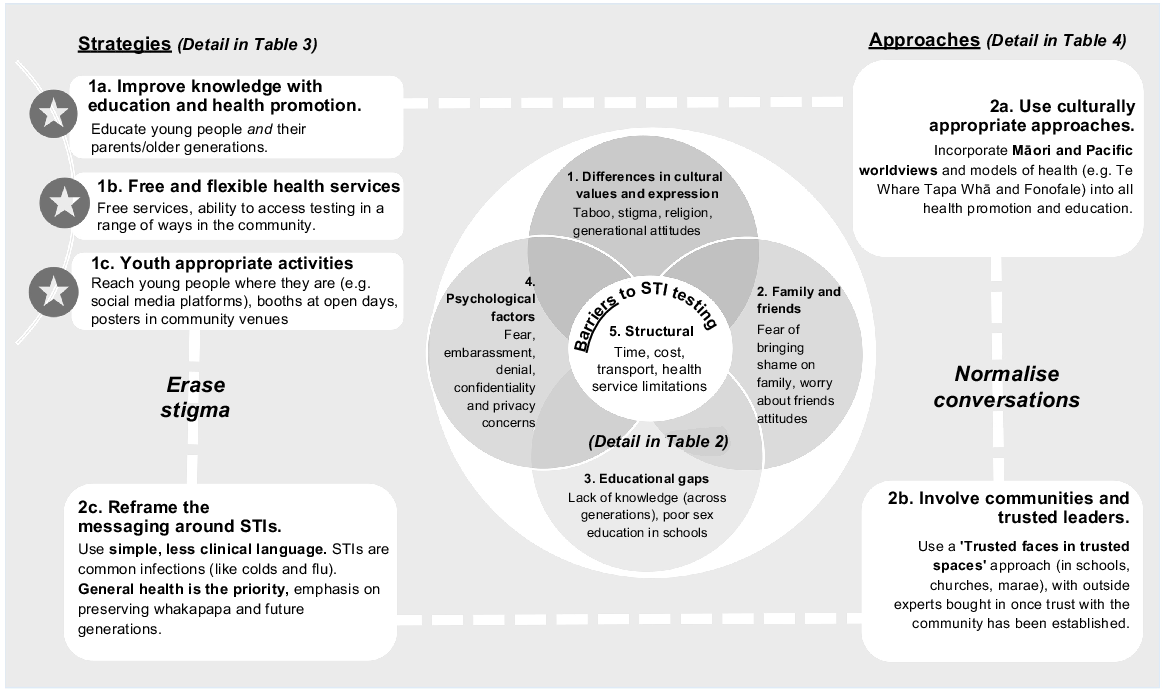
Fig. 2 summarises the overall findings from this work with the five themes identified as barriers to STI testing shown in the centre of the figure, and two main themes related to participants’ ideas about how to overcome some of these barriers depicted around the outside (Fig. 2). Table 2 summarises the barriers to STI testing that centred around five overlapping themes: differences in cultural values and expression, family and friends, educational gaps, psychological factors and structural obstacles. Cultural and family values are intertwined and in turn linked to educational gaps and psychological barriers.
Overview of study findings: participant-identified barriers to accessing STI testing and suggested strategies to overcome them.
Themes | Illustrative quotes | |
|---|---|---|
Theme 1. Differences in cultural values and expression | ‘It’s not within my culture to really talk about. It’s not what you talk about.’ (G4, M) ‘I don’t think it, it’s not even us, I mean we’re all good. The older generation where it was such a bad thing to have [an STI] back then, eh.’ (G1, F2) ‘It’s not a subject you could talk to your parents about. Especially in the church, cos anything about this, to do with this, its hard. I talk to my sister more about these things cos she knows everything. I don’t talk to Mum about it.’ (G3, YP1) ‘Being in church the beliefs of our parents are really strongly embedded, and it just sucks. For me, that’s my parents, and having to talk about sex or anything, because we’re not married it’s a no-go. They’re strict in their cultural reasons as well. So it would be hard to overcome and hard to talk about.’ (G2, F) ‘I remember my Mum saying to me ‘you don’t use plugs, you use the nappies’ or you know, the pads. When I asked her why she said, ‘if you’re using your finger, then you’ve had a sex’ [laughter] (G2, F1) ‘Our point of view is different to our parents’ point of view. It might have been a taboo subject to talk about back in their day but in this day and age like, you wanna be able to talk to your parents. You might not feel comfortable but having your parents educated that times have changed, it is common to catch it now, kind of thing.’ (G1, F4) ‘When I started thinking about this stuff I went to my aunty, one of my real close aunties to help me get on like, birth control and stuff like that, as opposed to my mum.’ (G1, F1) ‘We are actually really comfortable within this space (the wānanga) that’s made it, the process of this a bit easier to actually talk about it. But if this was us at home? We’d be like, cringe (laughter)’ (G2, F) | |
Theme 2. Family and friends | ‘You don’t wanna put shame on your family.’ (G2, F) ‘You don’t want your family to know.’ (G3, F13) ‘Judgement. Pretty uncomfortable. Yeah’ (G3) ‘I think the biggest one here is the cultural barrier. Yeah, just umm, the fear of getting caught, if you see your family when you’re out. That’s probably the worst thing.’ (G2, F) ‘A lot of this generation will be first generation here in New Zealand. So their parents are from the Islands where none of this was…wasn’t a thing.’ (G2, F) ‘And just like inconvenient. Like if you can’t take yourselves to the doctors and you don’t want your parents to know. Then, it’s a problem.’ (G1, M). ‘Your friends might laugh at you.’ (G3, M) | |
Theme 3. Educational gaps | ‘Education, especially it’s shit in school, I didn’t learn anything.’ (G1, F3) ‘Don’t know where to go. Not easily accessible here.’ (G3) ‘Yeah, I didn’t know this stuff on the screen [Facts about STIs] it’s another planet.’ (G1, M) ‘I feel like there’s just not enough awareness around the resources that are available to younger people.’ (G4, F) ‘So many women wouldn’t know just by getting an STI and like not doing anything about it…[results in] not having children.’ (G1, F) ‘I wouldn’t go to my Mum and say oh come help me take a gonorrhea test, cos she’ll be like oh, what’s that?’ (G2, F3) | |
Theme 4. Psychological factors | ‘It’s kind like, why is there such a stigma around it, though? It’s something so common. Why is it so…bad?’ (G1, F4) ‘The barrier of going into a clinic and asking for a test and being asked are you sexually active? We don’t want to be asked too many questions from staff. Otherwise, we will seek health services elsewhere.’ (G2) ‘Denial, yeah, embarrassment and denial.’ (G3) ‘Probably even just too scared, just better not knowing. Denial.’ (G1, F2) ‘Uncomfortable showing your parts.’ (G4, F) ‘Fear of knowing that you actually need to get tested.’ (G2) ‘Yeah cos a lot of people, like our community all know each other. Yeah you can’t do anything around here [laughter]. You can’t get away with anything.’ (G2, YP) [re. school nurses] ‘It’s too, like, local.… you see her every day. Just a lack of privacy with some school nurses. They talk to students.’ (G4, F) ‘It’s just not a priority... and it’s not urgent, like, if we can’t solve a problem straight away then we’ll just leave it.’ (G1, F1) | |
Theme 5. Structural barriers | ‘Even school nurses though like, they’re not in every day, they only visit like, what, once a week, twice a week. Even that is inconvenient.’ (G1, F3) ‘Not many people know that there are free services out there.’ (G1, F) ‘Too expensive for people.’ (G2) ‘For the young ages if they can’t access a car then…’ (G2) ‘We’re working. You’re working. You don’t have enough time.’ (G4, M) |
When discussing potential ways to address some of the barriers, there were two main themes: (1) with content related to suggested strategies about ‘what’ could be done (described in Table 3); and (2) ideas about ‘how’ these strategies might be effectively delivered (described in Table 4). Conversations about ‘what’ touched on the need for free and flexible sexual health services, but with a primary focus on the importance of better education and health promotion for young people and their parents. A range of activities were suggested to reach youth ‘where they are’ (including use of social media platforms such as TikTok, as well as in church, marae and other community settings). Participants identified the need for strategies to be underpinned by culturally appropriate approaches relevant to their own (Māori and Pacific) worldviews. They felt that parental and community involvement were key and that reframing the narrative about STI testing was necessary to facilitate easier conversations. They suggested opening the way to improved knowledge and awareness about sexual health was an important way to reduce stigma. Feedback following group work in Group 1 included:
We think every strategy needs to be contributing to erasing the stigma, the bad stigma associated with this topic. (G1)
Theme 1. Strategies | Illustrative quotesA | |
|---|---|---|
(1a) Improve knowledge through education and health promotion | ‘In schools, promoting it through sex ed like programs, all they do at school is show them how to put a condom on – whoopdedoo.’ (G1, F) ‘Maybe, if you like, went into schools? they’ll pay more attention to it.’ (G4, F) ‘I think our main one was just educating our Polynesian parents, families.’ (G2, F3) ‘So yeah, just the experiences of our parents’ families, once they’re educated then we can be educated as well. Some of our parents don’t really know anything, they are learning with us.’ (G2) ‘Teaching our parents like, inevitably young people are gonna have sex so if parents know safe, healthy practices to teach their young people and prevent, you know, health issues.’ (G1, M) | |
(1b) Free and flexible access | ‘It would be better if it was more accessible by being cheaper. And especially because we know now that 15–25-year-olds have the most STIs and they’re also the age bracket who don’t have the most money.’ (G1, F1) ‘Make it more accessible. And more testing options like, through schools, at home, or just like general drop-off locations wherever’. (G1, M) ‘Maybe going and having [tests together], might be cringe for others, but group testing like being able to go get tested with your best mate.’ (G1, F2) ‘Like doing those little pop-in pop-up stalls. Like when its open day, at polytechnics and universities, I’ve never seen an STD stand.’ (G2) | |
(1c) Use of ‘youth appropriate’ activities | ‘Good promotion and ask young people how to promote to young people (TikTok, workshops) and go to where the youth are.’ (G1 groupwork note) ‘You know, like TikTok, social media, um specially with the younger generation, always on TikTok doing their dances. You could make an STI song.’ (G1, M) ‘Start bringing the conversation into the schools, and then, also, going into churches, maraes and like, even gangs.’ (G1, M) ‘Use bright and bold colours, marketing, and ads on tv or the internet for those who are sexually active.’ (G4, F). ‘I feel like porn influencers would be a good one, like Only Fans.’ (G4, F) ‘If the target is to raise our awareness for the young ones, then social media is definitely a platform, not so much in schools because the majority of kids that actually need this weren’t going to school.’ (G2, F) |
Theme 2. Approaches | Illustrative quotesA | |
|---|---|---|
(2a) Use culturally appropriate approaches | ‘Parents getting together and arranging the best way to approach this, when we think about our culture we do everything as a whānau. If you want to engage with Māori and Pasifika you must have knowledge on their world and their culture.’ (G1, F1) ‘If I were to take it back to my iwi I’d probably tell them, to our Te Whare Tapa Whā [Māori model of health], for our tinana (body), like our body is our temple, we’ve got to look after it, cos there are long term affects as well, just bringing it up like could affect us having pēpē [babies] in the future.’ (G2, F) ‘But if we look at churches, we need to change the language and how we approach [this], being aware of the audience and context. So you wouldn’t go to a pastor and say we’re here to talk about, you know, sexually transmitted infections.’ (G2, F2) ‘We have a monthly session with our rainbow community. So there’s talanoa [conversation/discussion], we call it ‘Cocoa session’ or ‘Cocoa Night’, and that could be a session in there where you come and talk to our rainbow community and set one up for everybody else’. (G2, F1) | |
(2b) Involve communities and trusted leaders
| ‘I don’t wanna be talking about stuff to people who don’t understand the way I’ve been brought up in my culture.’ (G1, F1) ‘I think you, you would have to find the right people in the community.’ (G2, F) ‘Something that would resonate is more like Pacific Islanders, I feel like there’ll be a lot more influence, especially on our Pacific Communities, if more people that like looked like me, were encouraging me to like do the test.’ (G4, F) ‘Approach the leaders and influencers... Like the head boys, the main influencers in the school.’ (G1, F1) ‘Another way with the church is to approach the youth leaders, because they’re so familiar with the church it becomes their job to deliver it to parents, the Deacon and, and say ‘we need this for our kids, our youth’. They become advocates for youths, to advocate to the older lot, which makes it easier for people to come in to deliver that [education].’ (G2) ‘I say, convince the pastor. Cos everyone always follows the pastor.’ (G2, M1). [Agreement in group] | |
(2c) Reframe the messaging to enable conversations
| ‘You just gotta think it’s a health thing. People talk about like, COVID…and that’s the thing, it’s an infection you know. So why is this any different?’ (G1, M) ‘And you know so, so, there’s a word ‘normalising.’ It’s like catching a cold.’ (G2, F1) ‘Even talking about sex like, is helping remove the stigma of it.’ (G1, F1) ‘It’s more like, ok we are just looking out for your health. So if we change the wording of STI, we already know it’s testing for an STI or whatever infection, but if we go towards a culture where we are primarily looking at your health. Your health is priority. So that’s just, using the right words to deliver that [message].’ (G2, F2). ‘Make it more common in conversations.’ (G1, F) ‘Yeah having sex is more like health-like, trying to be healthy.’ (G1, M1). ‘Yeah, talk about it in a healthy way, in a different way.’ (G1, F1) ‘And you know to our parents, any word that starts with ‘sex’ is like tapu [sacred]. So if you change that word to something that’s more approachable, that you could say in the church around the old people without them going ‘Ugh’ you know, something that I could say to my kids without them cringing, then it might be more approachable.’ (G2, F1) ‘But you don’t hear, you know if you’re active and you don’t test yourself, you might not have your generation will stop here. Your family line stops here.’ (G2, F1) |
Several participants drew on experience with community-led coronavirus disease 2019 (COVID-19) public health initiatives. For example, one participant raised the example of a successful social media campaign run by and for their community to promote vaccination. The implication was that this approach could also work to foster a culture where STI testing is considered important not just for the individual, but for their wider whānau (family):
We had young people who did these clips, and then people that you see at the food plaza or you know at the market, and they’re telling their stories, their reasons why they wanted to get the vaccine. And a lot of it, it wasn’t for selfish reasons, you know it wasn’t for their own personal self but for their whakapapa. (G2, F1)
Discussion
Māori and Pacific young people in this study identified barriers related to differences in cultural values, family and friends, educational gaps, psychological and structural factors as limiting access to STI testing. There was variability in knowledge about testing within and between groups but an overall desire to know more. Discussion about improving access to testing focused on the need for better education, health promotion, free and flexible options for STI testing. For Pacific participants, culture, religion and parental attitudes were identified as limiting their ability to talk and learn about sexual health in the context of family. They acknowledged that their understanding of sexual health could be strengthened if knowledge held by their parents, families and wider communities improved (‘learning together’). While speaking respectfully about the difficulty their parents and previous generations faced in talking about sexual health, they felt this contributed to lack of knowledge, and for Pacific peoples this was strongly linked with religious beliefs. However, they also wanted to challenge the status quo and work towards eliminating stigma using approaches that encompass their cultural values and beliefs.
Like other studies, participants reported psychological barriers (fear, shame, embarrassment, and confidentiality concerns), lack of knowledge (not knowing when, where or how to test) and structural factors (cost, lack of transport, service limitations) as key reasons they would not seek STI testing.17 These findings serve as a reminder to clinicians to offer opportunistic STI testing to young people, explaining why it is important, what is involved and reiterating the confidential nature of patient–provider interactions. Past studies exploring barriers to STI testing have included few Māori or Pacific participants, so concerns related to parents, family and culture have not explicitly been reported as barriers in the context of STI testing. Pacific participants acknowledged limitations related to their strong church ties, but also saw opportunities to involve church youth leaders and communities in the development and delivery of education and health promotion. Several participants noted a desire to talk to parents about sexual health, but that it was challenging so instead they relied on sisters or aunties as reliable, trusted sources of information. A past study involving Niuean young people in NZ also highlighted the role sisters play in passing on information about sexual health.27 Some of our findings are consistent with those of an online survey that involved 81 Pacific university students (most aged 18–27 years). For example, cultural values were identified by the University students as a barrier to open conversation about sexuality and reproduction in a way that hinders knowledge-sharing between generations.28 The study authors concluded that ‘Pacific young people desire to speak more openly and freely about sex, relationships, sexuality and reproduction, indicative of the unique needs of a new generation of Pacific Aotearoa young people’.28 This viewpoint closely reflects the views of Pacific young people in the current study.
Both Māori and Pacific participants said they wanted education and health promotion strategies to be delivered using ‘culturally appropriate’ approaches. For example, they suggested engaging trusted community members to deliver messages that incorporate their worldviews and holistic models of wellbeing, citing Te Whare Tapa Whā26 and the Fonofale Model of Health as examples.25 One participant referenced a successful community COVID-19 vaccination initiative in which vaccination was framed as a way to protect whānau and community health; an approach they thought could be applied to STI testing. Participants felt that considering STIs as just another common infection (such as COVID-19, colds or flu) could also help normalise conversations and promote measures to tackle them.
Incorporating cultural values and beliefs into sexual health education was viewed as having potential to create social change, normalising conversations about sexual health between young and older generations. As examples, rather than thinking about sexual health as a stand-alone issue, participants wanted a more holistic view where it is considered part of general health and wellbeing, an approach they felt would help reduce associated shame and stigma. Understanding the potential impact of untreated STIs on future fertility resonated with participants as an important reason for getting tested. Whakapapa (or identity, genealogy, family lineage) is fundamental to Māori health and wellbeing, so preventing or reducing the spread of STIs is vital for the protection of fertility and preservation of whakapapa.2 Similarly, for Pacific peoples, family is the foundation that underpins all aspects of health and wellbeing, so preservation of reproductive health is central to maintenance of family and community wellbeing.
Participants articulated how education and health promotion activities should be framed. These approaches closely align with Māori and Pacific frameworks of health promotion21,29 and the 2020 Relationships and Sexuality Education (RSE) curriculum guide for years 9–13.30 However, RSE and health promotion activities are clearly not being delivered in a way that effectively reaches Māori and Pacific young people. RSE is not taught consistently in terms of content, quality or quantity in Aotearoa. A national survey of teachers in 2022 reported low levels of confidence integrating mātauranga Māori (Māori knowledge) and other cultural knowledge perspectives into their RSE teaching, and most schools fall short of the recommended annual minimum of 12–15 taught hours.31 Similarly, the health promotion workforce in Aotearoa is fragmented and under-resourced, and sexual health is often overlooked as other youth health issues such as mental health, drug and alcohol harm reduction are prioritised.32 The need for evidence-based Māori and priority population-led health promotion initiatives to reduce STIs has been identified as a priority area in the Aotearoa New Zealand Sexually Transmitted and Blood Borne Infection (STBBI) Strategy 2023–2030.22 The ideas identified in this study could be further developed and incorporated into community-led health promotion activities to equip Māori and Pacific young people (and their whānau) with the knowledge they need to support sexual health care.
Strengths and limitations
This is the first qualitative exploration of barriers facing Māori and Pacific young peoples’ access to STI testing and highlights ways in which some of these barriers could be addressed. Our recruitment method was a strength of the study. By gaining support from community-based youth organisations that had strong existing links to groups of young people, we reached a diverse mix of participants inclusive of Māori and Pacific, a mix of genders and sexual orientations, as well as participants who were NEET. The four meetings proceeded as planned with all participants who had signed up attending, which is testament to the valuable work our supporting organisations undertake for rangatahi in their communities. Participants were given giftcards in the spirit of reciprocity to acknowledge their time and the knowledge they shared, which likely added to their motivation to participate. Care was taken to ensure participants would feel willing and able to share views on the topic, by meeting in venues that were convenient and familiar, many participants already knew or knew of each other, or were from the same geographical communities. Participants were involved in setting the group kawa (culture) and shared ideas upfront about what was or was not acceptable. Food was shared, and karakia used to open and close the meetings. We observed that humour and shared laughter were common among participants throughout the wānanga, perhaps serving as a tool to overcome embarrassment or awkwardness and to foster a relaxed environment.33 Overall, participants were engaged and expressed curiosity about the topic as evidenced by a steady flow of conversation and ideas. Knowledge-sharing went both ways; facilitators shared information about STI testing during the wānanga and a summary of research findings was disseminated to organisations and participants once data had been collated.
Limitations of the study include our inability to link the speaker identities to specific quotes. This meant we could not undertake detailed analysis of any differences or similarities in ideas in relation to gender or ethnicity. The absence of a male facilitator is likely to have limited the way male participants contributed to discussions (they were also in the minority in two groups). While participants agreed to participate in a mixed-gender group (organised by supporting community organisations), this may not align with some cultural preferences when it comes to talking about sexual health; this will potentially have impacted on some participant’s level of comfort and ability to openly share views. Our facilitators had no prior relationship with participants which might have made the topic easier to talk about for some participants, but more difficult for others. The views and experiences shared by this group of urban-dwelling Māori and (mostly Sāmoan) Pacific young people in one region of Aotearoa will not necessarily be reflective of those held by others. Participants in Groups 1 and 2 (the main contributors to the ‘ideas’ generation part of the wānanga) were mostly Pacific ethnicities, so the breadth of ideas incorporating Māori perspectives is likely to have been limited.
Conclusion
In this study, Māori and Pacific young people described factors that impede their ability to access STI testing, with complexities related to their cultural identities adding additional barriers over and above those experienced by their Pākehā peers. They identified a need for free, flexible services for STI testing, together with community-based education and health promotion that considers their values and worldviews. Participants suggested reframing messages about STIs to place emphasis on protection of general health, whānau and community wellbeing would help to normalise conversations, and over time could help reduce the long-held stigma that continues to surround sexual health. Addressing the barriers identified in this work is critical to eliminate the inequitable burden of STIs experienced by Māori and Pacific young people. Prioritising, resourcing and building a culturally capable workforce to design and deliver health promotion will help equip Māori and Pacific young people and their families with knowledge and skills to maintain good sexual health and wellbeing.
Data availability
Our dataset comprises audiorecordings and related transcripts as well as handwritten notes containing names and other identifiable information about participants. Raw data are not publicly available as study participants were not asked for permission for their data to be shared publicly, and ethical approval was not sought for data to be shared.
Declaration of funding
This research was funded by a Lotteries Health Research Grant (LHR-2022-185437, awarded for the period February 2022–July 2023). The funding body had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Acknowledgements
We thank the 38 participants who openly shared their views, concerns and ideas with us. We are grateful to the community organisations that provided us with the opportunity and venues to work with their rangatahi networks (Wesley Community Action and Te Roopu Tiakai Rangatahi, Ngā Uri o Whiti Te Rā Mai Le Moana Trust, Talent Rise and Youth Inspire). We acknowledge the assistance of Shelley Duffin (Sexual reproductive health educator and promotor, Kōkiri Marae) who facilitated engagement with rangatahi-focused community groups, and The 502 (Youth One Stop Shop) rangatahi engagement lead who linked us with one of the groups.
References
1 Family Planning New Zealand. The sexual and reproductive health and rights of young people in Aotearoa New Zealand; 2022. Available at https://sexualwellbeing.org.nz/about/equity-in-aotearoa/position-statements/reproductive-rights/ [verified 1 November 2023]
2 Tipene J, Green A. He Pukenga Korero: Rangatahi and STIs in the Waikato. Online report; 2017. Available at http://tewhariki.org.nz/assets/He-Pukenga-Korero-Final-Report-31-Aug-2017.pdf [verified 1 November 2023]
3 New Zealand Sexual Health Society. STI management guidelines for use in primary care; 2021. Available at http://sti.guidelines.org.nz/ [verified 1 November 2023]
4 Rowley J, Vander Hoorn S, Korenromp E, Low N, Unemo M, Abu-Raddad LJ, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ 2019; 97(8): 548-62P.
| Crossref | Google Scholar | PubMed |
5 Price MJ, Ades AE, Soldan K, Welton NJ, Macleod J, Simms I, et al. The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis. Health Technol Assess 2016; 20(22): 1-250.
| Crossref | Google Scholar | PubMed |
6 New Zealand Sexual Health Society. Syphilis in pregnancy. Antenatal management guidelines for maternal and congenital syphilis; 2020. Available at https://www.nzshs.org/docman/guidelines/management-of-sexual-health-conditions/syphilis/syphilis-in-pregnancy/397-syphilis-in-pregnancy-v1-sep-2020/file [verified 1 November 2023]
7 The Institute of Environmental Science and Research Ltd. New Zealand sexually transmitted infection (STI) surveillance dashboard; 2023. Available at https://www.esr.cri.nz/our-research/nga-kete/infectious-disease-intelligence/sexually-transmitted-infection-sti-surveillance/ [verified 1 November 2023]
8 Manatū Hauora Ministry of Health. Sexual and reproductive health – STI testing coverage for 15–24 years olds; 2021. Available at https://nsfl.health.govt.nz/dhb-planning-package/system-level-measures-framework/data-support-system-level-measures/youth-slm--4 [verified 1 November 2023]
9 Te Puawai Tapu. To Tatou Hokakatanga: Action and Intervention in Sexual and Reproductive Health. A Report Prepared for the Health Research Council of New Zealand; 2007. Available at https://teatawhai.maori.nz/research-projects/to-tatou-hokakatanga-action-and-intervention-in-sexual-and-reproductive-health/ [verified 11 March 2024]
10 Institute of Environmental Science and Research Limited. Sexually transmitted infections in New Zealand: supplementary annual surveillance report; 2023. Available at www.esr.cri.nz/digital-library/sexually-transmitted-infections-annual-surveillance-report-2022/ [verified 1 November 2023]
11 Health Quality & Safety Commission. A window on the quality of Aotearoa New Zealand’s health care 2019 – a view on Māori health equity | He matapihi ki te kounga o ngā manaakitanga ā-hauora o Aotearoa 2019 – he tirohanga ki te ōritenga hauora o te Māori; 2019. Available at https://www.hqsc.govt.nz/assets/Our-data/Publications-resources/Window_2019_web_final-v2.pdf [verified 1 November 2023]
12 New Zealand Sexual Health Society. STI guidelines: Māori sexual health framework; 2021. Available at https://sti.guidelines.org.nz/maori-sexual-health-framework/ [verified 1 November 2023]
13 McDonagh LK, Saunders JM, Cassell J, Curtis T, Bastaki H, Hartney T, et al. Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: a systematic review. Implement Sci 2018; 13(1): 130.
| Crossref | Google Scholar |
14 Bender SS, Fulbright YK. Content analysis: a review of perceived barriers to sexual and reproductive health services by young people. Eur J Contracept Reprod Health Care 2013; 18(3): 159-67.
| Crossref | Google Scholar |
15 Kennedy EC, Bulu S, Harris J, Humphreys D, Malverus J, Gray NJ. “Be kind to young people so they feel at home”: a qualitative study of adolescents’ and service providers’ perceptions of youth-friendly sexual and reproductive health services in Vanuatu. BMC Health Serv Res 2013; 13: 455.
| Crossref | Google Scholar |
16 Newton-Levinson A, Leichliter JS, Chandra-Mouli V. Sexually transmitted infection services for adolescents and youth in low- and middle-income countries: perceived and experienced barriers to accessing care. J Adolesc Health 2016; 59(1): 7-16.
| Crossref | Google Scholar |
17 Denison HJ, Bromhead C, Grainger R, Dennison EM, Jutel A. Barriers to sexually transmitted infection testing in New Zealand: a qualitative study. Aust N Z J Public Health 2017; 41(4): 432-7.
| Crossref | Google Scholar |
18 Rose SB, Garrett SM, McKinlay EM, Morgan SJ. Experience of sexual healthcare by Māori and non-Māori young people: an online survey of 15–24 year olds in Hawkes Bay, New Zealand. Int J Sex Health 2022; 34(1): 118-29.
| Crossref | Google Scholar |
19 Rose SB, Garrett SM, McKinlay EM, Morgan SJ. ‘Be nice to us, we’re still learning’: an online survey of young people in Hawkes Bay, New Zealand, about unmet need for sexual health care and improving access to services. Sex Health 2021; 18: 394-404.
| Crossref | Google Scholar |
20 Green A, Waiti J. Planning a national STI website that appeals to young Māori; 2014. Available at https://tewhariki.org.nz/assets/stief-project-report-and-appendices-2014-for-distribution.pdf [verified 1 November 2023]
21 Veukiso-Ulugia A. Best practice framework for the delivery of sexual health promotion services to Pacific communities in New Zealand. Report prepared for the Ministry of Health; 2013. Available at https://tewhariki.org.nz/assets/best-practice-sexual-health-framework-for-pacific-people-final-170kb.pdf [verified 1 November 2023]
22 Ministry of Health. Aotearoa New Zealand sexually transmitted and blood borne infection strategy 2023–2030. Wellington: Ministry of Health; 2023. Available at https://www.health.govt.nz/publication/aotearoa-new-zealand-sexually-transmitted-and-blood-borne-infection-strategy-2023-2030 [verified 1 November 2023]
23 Rose SB, Gardiner T, Dunlop A, Cole M, Garrett SM, McKinlay EM. Māori and Pacific young people’s perspectives on testing for sexually transmitted infections via an online service: a qualitative study. J Prim Health Care 2024;
| Crossref | Google Scholar |
24 Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006; 3(2): 77-101.
| Crossref | Google Scholar |
25 Pulotu-Endemann K. Fonofale model of health. In: Ministry of Health, editor. Strategic directions for the mental health services for Pacific Island people. Wellington: Ministry of Health; 1995. Available at https://d3n8a8pro7vhmx.cloudfront.net/actionpoint/pages/437/attachments/original/1534408956/Fonofalemodelexplanation.pdf?1534408956
26 Manatū Hauora Ministry of Health. Māori health models – Te Whare Tapa Whā (Mason Durie); 2017. Available at https://www.health.govt.nz/our-work/populations/maori-health/maori-health-models/maori-health-models-te-whare-tapa-wha [verified 1 November 2023]
27 Ikihele A, Nosa V. Mothers and sisters: educators of sexual health information among young Niue women born in New Zealand. Pac J Reprod Health 2019; 1(9): 513-20.
| Crossref | Google Scholar |
28 Young CD, Taumoepeau MM, Hohmann-Marriott BE, Girling JE, Bird RJ. Sexual and reproductive health knowledges: a study with Pacific young people enrolled in an Aotearoa New Zealand tertiary institution. Cult Health Sex 2024; 26: 265-83.
| Crossref | Google Scholar |
29 Green JA, Tipene J, Davis K. Mana Tangata Whenua: national guidelines for sexual and reproductive health promotion with Māori. First edition. Hamilton: Te Whāriki Takapou; 2016. Available at https://tewhariki.org.nz/assets/National_Guidelines_for_SRH_Promotion_with_Maori.pdf [verified 1 November 2023]
30 Ministry of Education. Relationships and sexuality education. A guide for teachers, leaders, and boards of trustees; 2020. Available at https://hpe.tki.org.nz/assets/healthpe/pdfs/RSE+Guide+y9-13.pdf [verified 1 November 2023]
31 Dixon R, Robertson J, Beliveau A, Reid S, Maitland R, Dalley J. New Zealand secondary school teachers’ perspectives on teaching relationships and sexuality education; 2022. Available at https://healtheducation.org.nz/wp-content/uploads/2022/11/RSE-secondary-teachers-experiences-full-report.pdf [verified 1 November 2023]
32 New Zealand Sexual Health Society. Request for action on the development of a national sexual health strategy and action plan; 2011. Available at https://www.nzshs.org/docman/about/nzshs-policy-submissions/188-development-of-a-sexual-health-strategy-and-action-plan [verified 1 November 2023]
33 Allen L. Don’t forget, Thursday is test[icle] time! The use of humour in sexuality education. Sex Educ 2014; 14(4): 387-99.
| Crossref | Google Scholar |