

Supporting healthcare professionals to offer reproductive genetic carrier screening: a behaviour change theory approach
Stephanie Best A B C D E * , Janet C. Long A , Zoe Fehlberg A B , Alison D. Archibald F G H and Jeffrey Braithwaite A
A B C D E * , Janet C. Long A , Zoe Fehlberg A B , Alison D. Archibald F G H and Jeffrey Braithwaite A
A Australian Institute of Heath Innovation, Macquarie University, Sydney, NSW 2113, Australia.
B Australian Genomics, Murdoch Children’s Research Institute, Melbourne, Vic. 3052, Australia.
C Peter MacCallum Cancer Centre, Melbourne, Vic. 3000, Australia.
D Victorian Comprehensive Cancer Centre Alliance, Melbourne, Vic. 3000, Australia.
E Sir Peter MacCallum Department of Oncology, University of Melbourne, Melbourne, Vic. 3000, Australia.
F Department of Paediatrics, University of Melbourne, Melbourne, Vic. 3000, Australia.
G Victorian Clinical Genetics Services, Murdoch Children’s Research Institute, Melbourne, Vic. 3052, Australia.
H Genomics in Society, Murdoch Children’s Research Institute, Melbourne, Vic. 3052, Australia.
Australian Journal of Primary Health 29(5) 480-489 https://doi.org/10.1071/PY23022
Submitted: 10 February 2023 Accepted: 12 April 2023 Published: 9 May 2023
Abstract
As reproductive genetic carrier screening (RGCS) becomes more widely accessible, ensuring uptake by primary healthcare professionals (HCPs) is essential to equitable service provision. This study aimed to identify and prioritise implementation strategies to reduce barriers and support HCPs to routinely offer RGCS in Australia.
HCPs (n = 990) involved in a large national research study, offering couples-based RGCS, were surveyed at three time points: prior to offering RGCS through the study (Survey 1: Barriers); 8+ weeks after offering to their patients (Survey 2: Possible supports); and towards the end of the study (Survey 3: Prioritised supports). HCPs were from primary care (e.g. general practice, midwifery) and tertiary care (e.g. fertility, genetics) settings. Results were analysed via a novel approach of using behaviour change theory (Capability, Opportunity and Motivation – COM.B) to align theory to practice.
Survey 1 (n = 599) identified four barrier themes: time constraints, lack of HCP knowledge and skill, patient receptivity, and HCP’s perceived value of RGCS. Survey 2 (n = 358) identified 31 supports that could facilitate HCPs offering RGCS. Survey 3 (n = 390) was analysed separately by speciality and clinic location. Prioritised supports for primary care HCPs were ‘regular continuing professional development activities’ and ‘a comprehensive website to direct patients for information’. There was general accordance with the perceived importance of the supports, although some difference in relation to funding between professional groups and clinic locations.
This study identified a range of supports acceptable to HCPs across specialties and geographic locations that policymakers may use to direct efforts to ensure the roll out of RGCS is equitable across Australia.
Keywords: behaviour change theory, COM-B, general practice, healthcare practitioners, implementation science, implementation strategies, Mackenzie’s Mission, reproductive genetic carrier screening.
Introduction
Reproductive genetic carrier screening (RGCS) is genetic testing which provides information to people about their chance of having children affected by an autosomal recessive or X-linked genetic condition. If a reproductive couple is found to have an ‘increased chance’ for offspring with a genetic condition there is usually a one in four chance of the condition for each child they have (Borry et al. 2017). This information can be used to inform reproductive decision-making. Historically, the international use of RGCS has been restricted to selected populations at elevated risk for one or a small number of conditions, and more recently has been accessed regardless of a priori risk on a user-pays basis (Henneman et al. 2016). In Australia, the cost of user-pays carrier screening for a 3-gene panel (cystic fibrosis, fragile X and spinal muscular atrophy) is between AUD350–400 and for an expanded panel AUD579–2200 (Leibowitz et al. 2022). There are Medicare items that cover part of the cost of carrier screening for select conditions and circumstances, with limited availability for tests requested by primary healthcare professionals. This current approach not only imposes a financial barrier but risks failing to identify most ‘increased chance’ couples because of the recessive nature of the conditions whereby most affected children are born to parents with no family history (Archibald et al. 2018). International and Australian peak bodies (The Royal Australian College of Obstetricians and Gynaecologists 2019; Royal Australian College of General Practitioners 2020) now recommend that information about RGCS is provided to all individuals planning a pregnancy or in early pregnancy.
Technological advances that enable multiple conditions to be screened at once, coupled with a reduction in costs, means that the integration of population wide RGCS programs in public health services is now feasible (van der Hout et al. 2017). Indeed, the Australian federal government has announced plans to make RGCS for cystic fibrosis, spinal muscular atrophy and fragile X syndrome freely available from late 2023 (Medical Services Advisory Committee 2020). In the lead up to this announcement, an Australian-wide research study known as Mackenzie’s Mission investigated how to make a RGCS program easily accessible to all people who wish to have it (Archibald et al. 2022).
RGCS is a complex health intervention dependant on the timely interplay between patients and clinicians during the pre-conception and antenatal period. A wide array of healthcare professionals (HCPs) can play a role in offering RGCS, e.g. primary care specialists, public/private obstetricians, fertility specialists and clinical geneticists. As RGCS moves into mainstream health care, primary care professionals such as general practitioners (GPs) and midwives will play an essential role in delivering equitable care (Delatycki et al. 2019). GPs recognise they are well placed to offer RGCS (Archibald et al. 2016; Best et al. 2022) as they already provide a suite of antenatal care, and are most likely to see a couple prior to conception which is the preferred timing of RGCS as it avails a greater number of reproductive options (Schuurmans et al. 2019). Yet compared to obstetricians, challenges to incorporating RGCS into routine clinical practice remain, and uptake amongst GPs is not high (Kizirian et al. 2019; Leibowitz et al. 2022). Known barriers to HCPs involve hurdles at various stages including lack of HCP knowledge and awareness, time constraints in appointments, a lack of patient resources and concerns about skills to deliver post-test counselling (Best et al. 2021).
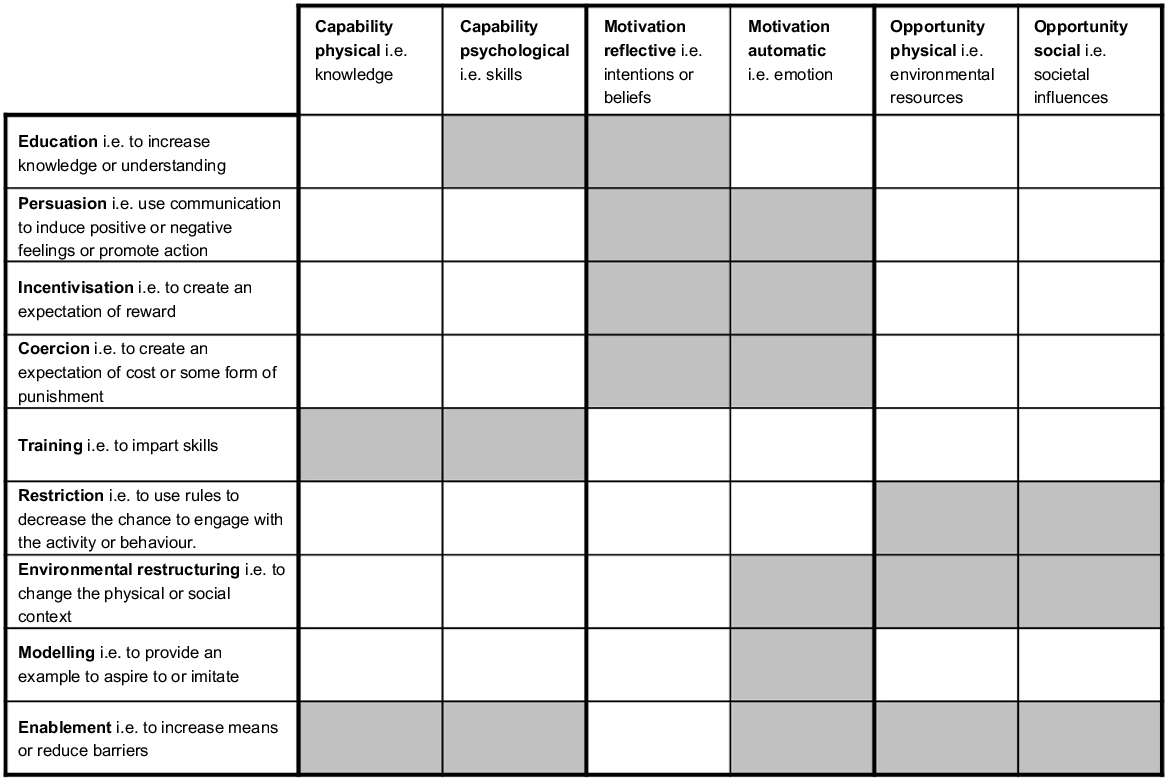
Incorporating RGCS into day-to-day practice requires a change in HCP behaviour. Given the complexity of RGCS and multi-level barriers, it is clear a targeted approach to support HCPs offering RCGS is required. Implementation science provides a rigorous mechanism to generate contextually specific strategies to promote the uptake of clinical evidence into routine practice (Bauer and Kirchner 2020). Theory-based implementation frameworks, when used to inform data collection and analysis, enables a stepwise approach to selecting and developing strategies that are supported by evidence. One framework that sits at the core of behaviour change is the COM-B (Michie et al. 2011). The COM-B argues that behaviour (B) is changed by modifying one or more of three factors: Capability (psychological and/or physical), Opportunity (societal and/or physical), and Motivation (automatic and/or reflective). Once identified, the relevant COM-B components can be mapped to a matrix (Fig. 1) and the intervention strategy(ies) that are likely to be appropriate and effective in addressing the barriers can be selected (Michie et al. 2011). In this study, we aimed to identify and prioritise implementation strategies to reduce barriers and enable HCPs, in particular those in primary care, to routinely offer RGCS.
COM-B Framework components with associated interventions – adapted from Michie et al. (2011). Key: Shaded boxes indicate effectiveness of an intervention by Capability, Opportunity or Motivation component.
Methods
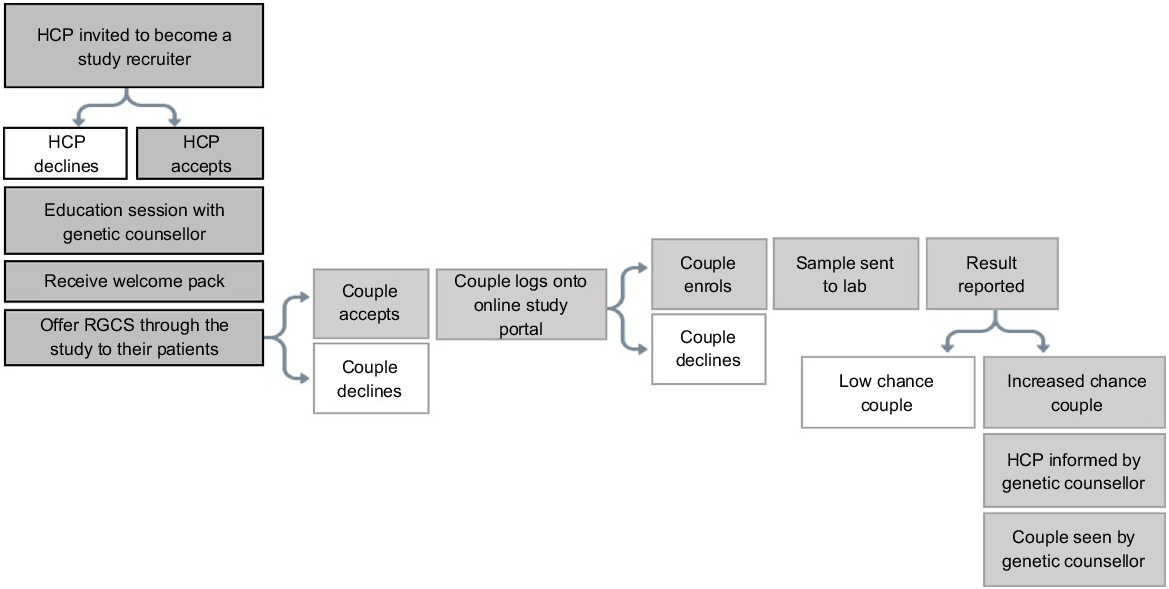
This survey study forms part of a larger implementation science programme that investigated influences on HCPs’ behaviour towards offering RGCS in the context of the Mackenzie’s Mission study. Mackenzie’s Mission was established as a couples-based screening program whereby reproductive couples, including individuals using gamete or embryo donors, were screened simultaneously. HCPs from various healthcare settings across Australia were invited by study genetic counsellors to become recruiters, and after completing an education session about RGCS and offering RGCS through the study, HCPs were able to offer RGCS to their patients who were planning or in early pregnancy. Once offered, couples could log onto an online portal, view education material, consent or decline testing and provide a mouth swab sample via the post to a participating laboratory for analysis. Couples would then receive their result online, or by a genetic counsellor if they were found to have an ‘increased chance’ of having children with a genetic condition. Fig. 2 illustrates the HCP and couple’s pathway to involvement in, and subsequent progression through, the Mackenzie’s Mission study. More details about Mackenzie’s Mission can be found in the literature (Archibald et al. 2022).
Pathway to participation in Mackenzie’s mission by healthcare professionals (HCPs) and couples.
For this study, HCPs involved in Mackenzie’s Mission (GPs, midwives, nurses, public/private obstetricians, fertility specialists, genetic counsellors and clinical geneticists) were invited to complete optional surveys at three time points throughout the programme. To accommodate the rolling recruitment of HCPs into the Mackenzie’s Mission study, Survey 1 and 2 were administered between February 2020 and November 2021 and Survey 3 between November 2021 and April 2022.
Surveys were completed online or in hardcopy, and data were stored online using REDCap software (see Table 1 for details). Survey 1 sought a range of HCP views on RGCS. To understand HCPs’ perceived barriers to offering RGCS prior to offering RGCS through the study we asked, ‘what do you think might deter HCPs from offering RGCS?’. Survey 2 captured HCP views after they had had an opportunity to offer RGCS. To identify possible supports derived from their experience of offering RGCS for approximately 8 weeks through the study we asked, ‘what would help you in offering RGCS?’. Together with 31 HCP interviews reported in detail elsewhere (Best et al. 2022), responses to the above question were collated to generate a list of potential ‘intuitive supports’ (i.e. practice-based enablers participants suggested) that may aid HCPs offering RGCS. To determine the priority of the ‘intuitive supports’, towards the conclusion of the Mackenzie’s Mission study, we asked HCPs to ‘rate how important the items would be in supporting them to offer RGCS, if they were provided ‘free of charge’ using a five-point Likert scale, ranging from ‘Not important at all’ to ‘Highly important’. Items were compulsory and pilot tested with the study genetic counsellors for comprehensibility.
| Timepoint | Eligibility | Mode | Aim | Question | |
|---|---|---|---|---|---|
| Survey 1 | All HCPs who expressed interest in becoming a study recruiter | Online and hard copy Invitation sent by study genetic counsellors No reminder sent | Identify perceived barriers to offering RGCS | What do you think might deter or stop healthcare professionals from offering RGCS? | |
| Survey 2 | All recruiting HCPs 8 weeks after completing the study education session | Online Invitation sent by research team Two-week reminder sent if survey was not completed | Identify potential supports to enable offering RGCS | What would help you in offering RGCS? | |
| Survey 3 | All recruiting HCPs who had been offering RGCS through the study for 12+ weeks | Online Invitation sent by research team Two-week reminder sent if survey was not completed | What potential supports are most important to healthcare professionals for future service delivery | Rate the importance of 31 intuitive supports for future service delivery |
RGCS, reproductive genetic carrier screening; HCP, health care professional.
Short answer responses (Survey 1 and 2) were analysed using inductive content analysis by experienced qualitative researchers (SB and ZF) (Vears and Gillam 2022) to identify perceived barriers and intuitive supports. Free text from 10 surveys was analysed independently before ZF completed the analysis. Fortnightly meetings were held (SB, ZF and JL) to discuss analysis, in particular for any challenging coding. Group discussions were used to classify frequently reported barriers and were further classified using the COM-B framework (Michie et al. 2011) to then link them with the associated highest ranking intuitive enablers (Fig. 1). For example, barriers associated with the COM-B code ‘physical capability’ i.e. knowledge, can be facilitated by training or enabling interventions e.g. facilitating access to knowledge. Quantitative survey data (Survey 3) were analysed through descriptive statistics using STATA ver. 12 (StataCorp LP) with results from the end of study survey prepared separately for primary care (GPs, GP/obstetricians, midwives and nurses) and tertiary care (clinical geneticists, genetic counsellors, obstetricians and fertility specialists) and further by clinic location. During analysis, the five-point Likert scale was collapsed into three categories ‘important’, ‘neutral’ and ‘not important’.
Results
Of the 990 HCPs who became study recruiters, a total of 599 HCPs (60% of the cohort) responded to Survey 1 and 358 HCPs (36% of the cohort) responded to Survey 2. Accounting for HCPs who had withdrawn from the study, of the 864 HCPs invited to complete Survey 3, 390 responses were received (45% of the cohort). Table 2 summarises the characteristics of survey respondents. Participants across the three time points were predominantly GPs based in metropolitan areas across Australia, comparable to the distribution of the Australian population with 28% of Australians living in regional or remote areas (Australian Institute of Health Welfare 2022). Prior to Mackenzie’s Mission, 74% of HCPs had previous experience offering RGCS. By the end of the study, on average, HCPs had been offering RGCS through Mackenzie’s Mission for around 1 year (55 weeks), however this ranged greatly from 14 to 100+ weeks. Most HCPs (46%) offered RGCS at least once a month, whereas 38% offered RGCS more frequently (weekly or daily).
| HCP – characteristics, n (%) | Survey 1 (n = 599) | Survey 2 (n = 358) | Survey 3 (n = 390) | |
|---|---|---|---|---|
| Primary care | ||||
| General practitioner | 407 (67.95) | 214 (59.61) | 241 (61.54) | |
| General practitioner/obstetrician | 14 (2.33) | 12 (3.34) | 10 (2.31) | |
| Midwife | 15 (2.50) | 8 (2.23) | 9 (2.31) | |
| Nurse | 4 (0.66) | 0 | 2 (0.51) | |
| Tertiary care | ||||
| Genetic counsellor | 52 (8.68) | 43 (11.98) | 41 (10.51) | |
| Obstetrician (public/private) | 58 (9.68) | 42 (11.73) | 39 (10.00) | |
| Clinical geneticist | 29 (4.84) | 27 (7.52) | 28 (7.18) | |
| Fertility specialist | 17 (2.84) | 21 (5.85) | 20 (5.13) | |
| Genetics or obstetrics registrar | 3 (0.50) | 1 (0.27) | 0 | |
| Clinic/service locationA | ||||
| Metropolitan | 446 (73.62) | 288 (80.22) | 304 (77.95) | |
| Inner regional | 120 (20.03) | 61 (16.99) | 59 (15.13) | |
| Outer regional | 32 (5.34) | 20 (5.57) | 25 (6.41) | |
| Remote | 1 (0.17) | 16 (4.46) | 2 (0.51) | |
| Australian State or Territory | ||||
| New South Wales | 137 (22.97) | 124 (34.54) | 119 (30.51) | |
| Victoria | 264 (44.07) | 94 (26.18) | 110 (28.21) | |
| Queensland | 82 (13.69) | 67 (18.66) | 81 (20.77) | |
| Western Australia | 49 (8.18) | 33 (9.19) | 37 (9.49) | |
| South Australia | 40 (6.68) | 32 (8.91) | 35 (8.97) | |
| Tasmania | 24 (4.01) | 7 (1.95) | 4 (1.03) | |
| Northern Territory | 3 (0.50) | 1 (0.28) | 3 (0.77) | |
| Australian Capital Territory | 0 | 1 (0.28) | 1 (0.26) | |
| Previous experience offering RGCS | 442 (73.76) | n/a | n/a | |
| Frequency of offering RGCS | n/a | n/a | ||
| Daily | 22 (5.64) | |||
| At least once a week | 127 (32.56) | |||
| At least once a month | 181 (46.41) | |||
| Less than once a month | 55 (14.10) | |||
| Not had the opportunity to | 5 (1.28) | |||
| Number of weeks recruiting, mean (min – max) | n/a | ≈8 | 54.87 (14–108) | |
RGCS, Reproductive genetic carrier screening; HCP, healthcare professional.
A72% live in major cities, 18% in inner regional area, 8.0% in outer regional areas, 1.9% in remote or very remote areas (Australian Institute of Health Welfare 2022).
Perceived barriers to offering RGCS (short answer responses) – before participating in Mackenzie’s Mission
Upon analysis of Survey 1, four perceived barrier areas to offering RGCS were identified and were associated with COM-B attributes. Quotes are provided accompanied by the participants’ profession and geographical location.
Time constraints during appointments (COM-B: Opportunity) The most prominent barrier reported by over half of respondents was time constraints during consults. HCPs noted challenges to remembering or to be able to fit in discussions around RGCS with already full workloads and competing priorities.
TIME! (GP, metro, New South Wales)
Sometimes [I] forget when really busy. My patients often come for a 15-minute appointment and a shopping list of issues, so some get forgotten/delayed, especially the preventative care that is not on patients list of health issues. (GP, metro, Victoria)
Low RGCS awareness and knowledge and skill to offer RGCS (COM-B: Capability) Half of respondents described low engagement with RGCS because of a lack of awareness and knowledge about RGCS including the processes involved and the limited availability of training or resources. Low confidence in their ability to provide pre- and post-test counselling was considered to further deter HCPs from engaging with RGCS.
The lack of training for GPs in this area. It becomes a non-priority because we don’t have the correct answers and lack confidence, we then avoid offering it. (GP, inner regional, New South Wales)
Lack of confidence and training to counsel patients about screened conditions and abnormal results. (GP, metro, South Australia)
Patient receptivity and behaviour (COM-B: Opportunity) Patient factors reported by some respondents included: a lack of patient awareness or interest, and not seeking pre-conception advice. The cost of screening was often reported by respondents as the determining factor in patients’ decision-making and influenced who HCPs offered RGCS to with HCPs more likely to offer when they think there will be a positive uptake.
Doctors might make assumptions about what their [patient] can afford. Might be more likely to offer it in an affluent setting than in a lower socioeconomic setting. (GP, metro, Victoria)
HCP attitudes towards and beliefs about RGCS (COM-B: Motivation) Less prominent were respondents who felt HCPs’ beliefs about RGCS were a barrier: including the undecided ‘value’ of RGCS; not wanting to deliver ‘bad news’; beliefs about negative consequences for patients (i.e. increased anxiety); and religious or ethical considerations, especially around termination of pregnancy (TOP).
Philosophical objection to offering TOP as an option if genetic screening uncovers an issue. (GP, outer regional, Queensland)
Wondering whether it is overall beneficial to patients (unproven benefit). (GP, metro, Victoria)
Priorities for future supports
Thirty-one intuitive supports were identified (see Supplementary material 1) from the open text responses in Survey 2 and the HCP interviews. Table 3 presents the intuitive supports in order of their perceived importance by primary HCPs, not in order of appearance in the survey. Of the 31 intuitive supports presented to primary HCPs, 22 (70%) were considered ‘important’ by 75% or more of respondents. The most important, as endorsed by all but one primary HCP was ‘regular CPD activities’. Ninety-eight percent of respondents considered ‘a comprehensive website to direct patients for information’ and ‘funding screening which includes the cost of genetic counselling for ‘increased chance’ couples’ important. Also highly endorsed by 97% of respondents was ‘being part of a RGCS special interest group’ and ‘information on clear referral pathways for ongoing care’. The lowest scoring supports considered important by less than half of respondents were: ‘administrative support (e.g. coordination of results, billing patients)’, ‘promotion of RGCS within professional health networks’ and ‘receiving a regular newsletter’ or a ‘picture/story-based waiting room poster’.
| Intuitive supports, n (%) (n = 262) | COM-B intervention | Important | Neutral | Not important | |
|---|---|---|---|---|---|
| Regular CPD activities | Education training | 261 (99.62) | 1 (0.38) | 0 | |
| A comprehensive website to direct patients for information | Env restructure | 258 (98.47) | 4 (1.53) | 0 | |
| Funding screening which includes the cost of genetic counselling for ‘increased chance’ couples | Enablement | 257 (98.09) | 5 (1.91) | 0 | |
| Being part of a RGCS special interest group | Modelling | 246 (97.71) | 6 (2.29) | 0 | |
| Information on clear referral pathways for ongoing care | Education | 256 (97.71) | 3 (1.15) | 3 (1.15) | |
| RGCS screening integrated into your practice’s electronic system (e.g. test request forms and reporting) | Env restructure | 255 (97.33) | 5 (1.91) | 2 (0.76) | |
| Accessible information on common genetic conditions screened | Education | 253 (96.56) | 6 (2.29) | 3 (1.15) | |
| Printed information sheet to give to patients | Env restructure | 251 (95.80) | 7 (2.67) | 4 (1.53) | |
| Notification when a couple has provided samples | Env restructure | 248 (94.66) | 11 (4.20) | 3 (1.15) | |
| Funding for longer consultations | Enablement | 247 (94.27) | 11 (4.20) | 4 (1.53) | |
| Resources that contain visual explanations of RGCS for patients | Env restructure | 242 (92.37) | 19 (7.25) | 1 (0.38) | |
| Having the contact details of a genetic counsellor | Enablement | 234 (89.31) | 26 (9.92) | 2 (0.76) | |
| Receiving a check-in call from a genetic counsellor | Enablement | 233 (88.93) | 27 (10.31) | 2 (0.76) | |
| Funding for additional services (e.g. pre-implantation genetic testing, IVF) | Enablement | 235 (89.69) | 21 (8.02) | 6 (2.29) | |
| Information on other preconception or antenatal genetic tests | Education | 230 (87.79) | 29 (11.07) | 3 (1.15) | |
| Easy referral pathways to genetic services | Enablement | 229 (87.40) | 27 (10.31) | 6 (2.29) | |
| Having a genetic counsellor deliver ‘increased chance’ results | Enablement | 226 (86.26) | 28 (10.69) | 8 (3.05) | |
| Incorporating offering RGCS into routine care for antenatal or pre-pregnancy planning appointments | Env restructure | 217 (82.82) | 35 (13.36) | 10 (3.82) | |
| Translated resources for patients | Env restructure | 214 (81.68) | 31 (11.83) | 17 (6.49) | |
| Accessible information on all genetic conditions screened | Education | 209 (79.77) | 42 (16.03) | 11 (4.20) | |
| Being able to contact a genetic counsellor you know | Enablement | 203 (77.48) | 52 (19.85) | 7 (2.67) | |
| A short video to show patients explaining reproductive genetic carrier screening | Env restructure | 201 (76.72) | 50 (19.08) | 11 (4.20) | |
| Fast and reliable turnaround times for results | Env restructure | 194 (74.05) | 60 (22.90) | 8 (3.05) | |
| Wider awareness amongst your peers (within clinic and/or externally) | Persuasion | 191 (72.90) | 57 (21.56) | 14 (5.34) | |
| A RGCS community awareness campaign | Env restructure | 191 (72.90) | 54 (20.61) | 17 (6.49) | |
| Access to interpreters | Env restructure | 191 (72.90) | 44 (16.79) | 27 (10.31) | |
| Script to follow when introducing discussion around RGCS | Modelling | 145 (55.34) | 68 (25.95) | 49 (18.70) | |
| Picture/story-based waiting room posters | Env restructure | 124 (47.33) | 90 (34.35) | 48 (18.32) | |
| Promotion of RGCS within professional health networks | Education | 99 (37.79) | 121 (46.18) | 42 (16.03) | |
| Receiving a regular RGCS newsletter | Education | 104 (39.69) | 103 (39.31) | 55 (20.99) | |
| Administrative support (e.g. coordination of results, billing patients) | Enablement | 94 (35.88) | 119 (45.42) | 49 (18.70) |
RGCS, reproductive genetic carrier screening; HCP, healthcare professional; CPD, continuous professional development; Env, environment.
Among tertiary HCPs (Table 4), the top support was ‘being part of a RGCS special interest group’ (99%) followed by ‘funding for additional services (e.g. pre-implementation genetics, IVF)’ (96%). Equally important was ‘RGCS integrated into your practice’s electronic system (e.g. test request forms and reporting)’ (96%).
| Intuitive supports, n (%) (n = 128) | COM-B intervention | Important | Neutral | Not important | |
|---|---|---|---|---|---|
| Being part of a RGCS special interest group | Modelling | 127 (99.22) | 1 (0.78) | 0 | |
| Funding for additional services (e.g. pre-implantation genetic testing, IVF) | Enablement | 124 (96.88) | 4 (3.13) | 0 | |
| A comprehensive website to direct patients for information | Env restructure | 124 (96.88) | 3 (2.34) | 1 (0.78) | |
| RGCS integrated into your practice’s electronic system (e.g. test request forms and reporting) | Env restructure | 123 (96.09) | 4 (3.13) | 1 (0.78) | |
| Funding screening which includes the cost of genetic counselling for ‘increased chance’ couples | Enablement | 122 (95.31) | 5 (3.91) | 1 (0.78) |
Note: complete list available in supplementary information.
RGCS, reproductive genetic carrier screening; CPD, continuous professional development; Env, environmental.
Table 5 shows the top 10 intuitive supports as rated by 90% or more of both primary care HCPs working in metropolitan and regional/remote areas of Australia. The results indicate an accordance between the two groups, however ‘funding for longer consultations’ was more important among primary HCPs working in regional/remote areas (97% vs 93%).
| Intuitive supports, n (%) | COM-B intervention | Metropolitan primary care HCPs (n = 262) | Regional/remote primary care HCPs (n = 73) | |||||
|---|---|---|---|---|---|---|---|---|
| Important | Neutral | Not important | Important | Neutral | Not important | |||
| Regular CPD activities | Education training | 188 (99.47) | 1 (0.53) | 0 | 73 (100) | 0 | 0 | |
| A comprehensive website to direct patients for information | Env restructure | 187 (98.94) | 2 (1.06) | 0 | 71 (97.26) | 2 (2.74) | 0 | |
| Funding screening which includes the cost of genetic counselling for ‘increased chance’ couples | Enablement | 187 (98.94) | 2 (1.06) | 0 | 70 (95.89) | 3 (4.11) | 0 | |
| Information on clear referral pathways for ongoing care | Education | 186 (98.41) | 1 (0.53) | 2 (1.06) | 70 (95.89) | 2 (2.74) | 1 (1.37) | |
| Being part of a RGCS special interest group | Modelling | 185 (97.88) | 4 (2.12) | 0 | 71 (97.26) | 2 (2.74) | 0 | |
| RGCS integrated into your practice’s electronic system (e.g. test request forms and reporting) | Env restructure | 184 (97.35) | 3 (1.59) | 2 (1.06) | 71 (97.26) | 2 (2.74) | 0 | |
| Accessible information on common genetic conditions screened | Education | 183 (96.83) | 3 (1.59) | 3 (1.59) | 70 (95.89) | 3 (4.11) | 0 | |
| Printed information sheet to give to patients | Env restructure | 180 (95.24) | 5 (2.65) | 4 (2.12) | 71 (97.26) | 2 (2.74) | 0 | |
| Notification when a couple has provided samples | Env restructure | 178 (94.18) | 9 (4.76) | 2 (1.06) | 70 (95.89) | 2 (2.74) | 1 (1.37) | |
| Funding for longer consultations | Enablement | 176 (93.12) | 9 (4.76) | 4 (2.12) | 71 (97.26) | 2 (2.74) | 0 | |
Note: complete list provided in the supplementary information.
RGCS, reproductive genetic carrier screening; CPD, continuous professional development; Env, environmental; HCP, healthcare professionals.
Table 6 links the frequently reported barriers (i.e. low HCP skill, knowledge and awareness; time in consultations; patient receptivity) with the associated COM-B component (i.e. Capability – physical and psychological; Opportunity – physical and Opportunity – social) and top ranked intuitive enablers (i.e. regular CPD activities and a comprehensive website twice). To identify if the intuitive enablers aligned with theoretical enablers, a further connection was made back to the COM-B framework (Fig. 1). Most of the intuitive enablers matched with theory, however, several highly ranked intuitive enablers did not match including, e.g. ‘funding screening which includes the cost of genetic counselling for ‘increased chance’ couples’ for primary care HCPs and ‘funding for additional services (e.g. pre-implementation genetics, IVF)’ for tertiary care HCPs.
| Top ranked barriers | COM-B component | Top ranked intuitive enablers linked to associated barriers | Alignment with COM-B intervention (Fig. 1) | |
|---|---|---|---|---|
| Low HCP skill, knowledge, awareness | Capability – physical and psychological | Regular CPD activities | Yes: Education and training | |
| Time in consultations | Opportunity – physical | A comprehensive website to direct patients for information | Yes: Env restructuring | |
| Patient receptivity | Opportunity – social | A comprehensive website to direct patients for information | Yes: Env restructuring | |
| HCP attitudes/beliefs | Motivation – reflective and automatic | Being part of a RGCS special interest group | Yes: Modelling |
HCP, healthcare professionals; CPD, continuous professional development; Env, environmental.
Discussion
Four common concerns to offering RGCS were reported by HCPs before participating in Mackenzie’s Mission: low HCP skill, knowledge and/or awareness of RGCS; additional time required in consultations; the potential for patients to be unreceptive to RGCS; and HCP attitudes and beliefs about RGCS. These findings provide support for, and offer an extended analysis to advance, previous studies in this field (Best et al. 2021). Participants suggested 31 intuitive enablers to facilitate offering RGCS with both primary and tertiary care HCPs in agreement with some of the highest ranked i.e. regular CPD activities, a comprehensive website to direct patients to for further information on RGCS, and being part of a RGCS special interest group. Other enablers varied e.g. funding: primary care HCPs placed a higher priority on the need for screening to include genetic counselling for ‘increased chance’ couples. In previous studies, GPs have been identified as the ideal professionals to be offering counselling (Poppelaars et al. 2003) although needing additional training (Schuurmans et al. 2019). Of interest is that 86% of primary care HCPs wanted genetic counsellors to deliver increased chance results, suggesting that funding for counselling is related to equitable service provision. In contrast, tertiary care participants wanted to see additional services such as in vitro fertilisation (IVF). The support required for metro and regional/rural primary care HCPs to offer RGCS is an under-researched field and while our study demonstrates that many enablers were common across the piece, those working in regional/remote areas prioritised funding for longer consultations.
Drawing on behaviour change theory, the four reported barriers could be aligned with intuitive enablers (Table 6) (Taylor et al. 2020). Surprisingly, all these alignments tie in with COM-B evidence-based associated interventions of education and training, environmental restructuring and modelling, suggesting this is an efficient approach to identifying appropriate interventions to support HCPs to offer RGCS (Michie et al. 2011) that could have relevance to policy makers. Applying behaviour change theory to the development of enablers to support offering of RGCS can optimise HCP time by building on extant knowledge and so preventing the need to reinvent the wheel, provide information on how and why an intervention may (or may not) work and promote the use of theory informed intervention design and policy making (Bullock et al. 2021).
Some higher prioritised intuitive enablers did not match the reported barriers, i.e. primary care: funding screening to include genetic counselling for ‘increased chance’ couples; and specialty: additional services such as IVF and regional/remote, funding for longer consultations. This may reflect the data collection time points of barriers prior to offering RGCS. At the outset of a programme when barrier data are collected, priorities may centre on adoption and feasibility while later on, when enablers data are collected, priorities may shift to sustainability (Proctor et al. 2011). Funding for genetic testing has been established as a priority for some time (Holtkamp et al. 2017); however, our study reveals a more nuanced requirement for funding allocations across HCP specialities and locality. Although there is overlap, the needs of primary and tertiary HCPs are different and will require a differential policy response if the uptake of broad-based, including nationwide, RGCS is to be successfully implemented.
Our study moves away from anecdotal approaches to identifying clinicians’ needs (Mendelsohn 2021) and draws on rigorous methodology to ascertaining support for clinicians to offer RGCS. This study builds on the work of Leibowitz et al. (2022) who identify patterns in HCP participation in RGCS and here we provide theory and practice informed insights into the needs of Australian HCPs in order for them to routinely offer RGCS. As to limitations, response rates were impacted by the SARS-CoV-2 pandemic. The profile of our survey respondents largely mirrored the Australian population and while this is desirable it also means the absolute number of regional/remote responses were relatively few. This population would benefit from additional research to garner further insights into their individual challenges. Non-genetic HCPs such as practice nurses and midwives were poorly represented in this study and could be valuable future referrers for RGCS (Best et al. 2021). Our analysis included both primary and tertiary HCPs reflecting the study population. Further in-depth analysis could be gained by targeting specific specialists such as GPs.
All-in-all, in this study we have identified and prioritised implementation strategies to support how HCPs, in particular GPs, routinely offer RGCS in Australia. Although some enablers were found to be common across locality and speciality, such as a comprehensive website to direct patients to for information, there was a more nuanced picture of enablers that aligned with behaviour change theory. Funding in particular was requested for genetic counselling by primary care, additional services by specialty care and longer consultations by GPs in regional/remote areas. The significance of these findings is critical for policy makers if RGCS is to be widely adopted and thereby avoid the risk of inequitable service provision.
Data availability
The data that support this study will be shared upon reasonable request to the corresponding author.
Declaration of funding
The Australian Reproductive Genetic Carrier Screening Project (Mackenzie’s Mission) is funded by the Australian Government’s Medical Research Future Fund as part of the Genomics Health Futures Mission (GHFM), grant GHFM73390 (MRFF-G-Mackenzie’s Mission). The grant is administered by the Murdoch Children’s Research Institute through Australian Genomics.
References
Archibald AD, Hickerton CL, Wake SA, Jaques AM, Cohen J, Metcalfe SA (2016) “It gives them more options”: preferences for preconception genetic carrier screening for fragile X syndrome in primary healthcare. Journal of Community Genetics 7, 159-171.
| Crossref | Google Scholar |
Archibald AD, Smith MJ, Burgess T, Scarff KL, Elliott J, Hunt CE, Barns-Jenkins C, Holt C, Sandoval K, Siva Kumar V, Ward L, Allen EC, Collis SV, Cowie S, Francis D, Delatycki MB, Yiu EM, Massie RJ, Pertile MD, du Sart D, Bruno D, Amor DJ (2018) Reproductive genetic carrier screening for cystic fibrosis, fragile X syndrome, and spinal muscular atrophy in Australia: outcomes of 12,000 tests. Genetics in Medicine 20, 513-523.
| Crossref | Google Scholar |
Archibald AD, McClaren BJ, Caruana J, Tutty E, King EA, Halliday JL, Best S, Kanga-Parabia A, Bennetts BH, Cliffe CC, Madelli EO, Ho G, Liebelt J, Long JC, Braithwaite J, Kennedy J, Massie J, Emery JD, McGaughran J, Marum JE, Boggs K, Barlow-Stewart K, Burnett L, Dive L, Freeman L, Davis MR, Downes MJ, Wallis M, Ferrie MM, Pachter N, Scuffham PA, Casella R, Allcock RJN, Ong R, Edwards S, Righetti S, Lunke S, Lewis S, Walker SP, Boughtwood TF, Hardy T, Newson AJ, Kirk EP, Laing NG, Delatycki MB, The Mackenzie’s Mission Study Team (2022) The Australian reproductive genetic carrier screening project (Mackenzie’s mission): design and implementation. Journal of Personalized Medicine 12, 1781.
| Crossref | Google Scholar |
Australian Institute of Health Welfare (2022) Rural and remote health. AIHW, Canberra. Available at https://www.aihw.gov.au/reports/rural-remote-australians/rural-and-remote-health
Bauer MS, Kirchner J (2020) Implementation science: what is it and why should I care? Psychiatry Research 283, 112376.
| Crossref | Google Scholar |
Best S, Long J, Theodorou T, Hatem S, Lake R, Archibald A, Freeman L, Braithwaite J (2021) Health practitioners’ perceptions of the barriers and enablers to the implementation of reproductive genetic carrier screening: a systematic review. Prenatal Diagnosis 41, 708-719.
| Crossref | Google Scholar |
Best S, Long JC, Fehlberg Z, Theodorou T, Hatem S, Archibald A, Braithwaite J (2022) The more you do it, the easier it gets: using behaviour change theory to support health care professionals offering reproductive genetic carrier screening. European Journal of Human Genetics 31, 430-444.
| Crossref | Google Scholar |
Borry P, Cassiman J-J, Hulstaert F, Liebaers I, Mortier G, Peeters H, Van den Bulcke M, Van Nerom A, Van Oyen H, Verellen-Dumoulin C (2017) Expanded carrier screening in a reproductive context. Towards a responsible implementation in the healthcare system. Advisory Report of The Superior Health Council no. 9240. Available at https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/shc_advisoryreport_9240_carrier_screening.pdf
Bullock HL, Lavis JN, Wilson MG, Mulvale G, Miatello A (2021) Understanding the implementation of evidence-informed policies and practices from a policy perspective: a critical interpretive synthesis. Implementation Science 16, 18.
| Crossref | Google Scholar |
Delatycki MB, Laing NG, Moore SJ, Emery J, Archibald AD, Massie J, Kirk EP (2019) Preconception and antenatal carrier screening for genetic conditions: the critical role of general practitioners. Australian Journal of General Practice 48, 106-110.
| Crossref | Google Scholar |
Henneman L, Borry P, Chokoshvili D, Cornel MC, van El CG, Forzano F, Hall A, Howard HC, Janssens S, Kayserili H, Lakeman P, Lucassen A, Metcalfe SA, Vidmar L, de Wert G, Dondorp WJ, Peterlin B, on behalf of the European Society of Human Genetics (ESHG) (2016) Responsible implementation of expanded carrier screening. European Journal of Human Genetics 24, e1-e12.
| Crossref | Google Scholar |
Holtkamp KCA, Vos EM, Rigter T, Lakeman P, Henneman L, Cornel MC (2017) Stakeholder perspectives on the implementation of genetic carrier screening in a changing landscape. BMC Health Services Research 17, 146.
| Crossref | Google Scholar |
Kizirian NV, Black KI, Musgrave L, Hespe C, Gordon A (2019) Understanding and provision of preconception care by general practitioners. Australian and New Zealand Journal of Obstetrics and Gynaecology 59, 799-804.
| Crossref | Google Scholar |
Leibowitz R, Lewis S, Emery J, Massie J, Smith M, Delatycki M, Archibald A (2022) Reproductive genetic carrier screening for cystic fibrosis, fragile X syndrome and spinal muscular atrophy: patterns of community and healthcare provider participation in a Victorian screening program. Australian Journal of Primary Health 28, 580-587.
| Crossref | Google Scholar |
Medical Services Advisory Committee (2020) Reproductive carrier screening for fragile X syndrome, spinal muscular atrophy and cystic fibrosis. Available at http://www.msac.gov.au/internet/msac/publishing.nsf/Content/1573-public
Mendelsohn BA (2021) Expanded carrier screening and the complexity of implementation. Obstetrics & Gynecology 137, 959-960.
| Crossref | Google Scholar |
Michie S, van Stralen MM, West R (2011) The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implementation Science 6, 42.
| Crossref | Google Scholar |
Poppelaars FAM, Henneman L, Adèr HJ, Cornel MC, Hermens RPMG, van Der Wal G, ten Kate LP (2003) How should preconceptional cystic fibrosis carrier screening be provided? Opinions of potential providers and the target population. Community Genetics 6, 157-165.
| Crossref | Google Scholar |
Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, Griffey R, Hensley M (2011) Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health and Mental Health Services Research 38, 65-76.
| Crossref | Google Scholar |
Royal Australian College of General Practitioners (2020) Genomics in general practice. RACGP, East Melbourne, Victoria. Available at https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/genomics-in-general-practice/genomics-in-general-practice/background [Accessed July 2022]
Schuurmans J, Birnie E, van den Heuvel LM, Plantinga M, Lucassen A, van der Kolk DM, Abbott KM, Ranchor AV, Diemers AD, van Langen IM (2019) Feasibility of couple-based expanded carrier screening offered by general practitioners. European Journal of Human Genetics 27, 691-700.
| Crossref | Google Scholar |
Taylor N, Healey E, Morrow A, Greening S, Wakefield CE, Warwick L, Williams R, Tucker KM (2020) Aligning intuition and theory: enhancing the replicability of behaviour change interventions in cancer genetics. Implementation Science Communications 1, 90.
| Crossref | Google Scholar |
The Royal Australian College of Obstetricians and Gynaecologists (2019) genomics advisory working group and women’s health committee. Genetic carrier screening (C-Obs 63). RANZCOG, Melbourne, Victoria. Available at https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical-Obstetrics/Genetic-carrier-screening(C-Obs-63)New-March-2019_1.pdf?ext=.pdf [Accessed July 2022]
van der Hout S, Holtkamp KCA, Henneman L, de Wert G, Dondorp WJ (2017) Advantages of expanded universal carrier screening: what is at stake? European Journal of Human Genetics 25, 17.
| Crossref | Google Scholar |
Vears DF, Gillam L (2022) Inductive content analysis: a guide for beginning qualitative researchers. Focus on Health Professional Education: A Multi-Professional Journal 23, 111-127.
| Crossref | Google Scholar |